Open pneumothorax surgery. Emergency care for closed and open pneumothorax
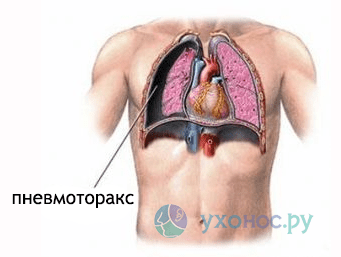
Pneumothorax is a pathology characterized by the accumulation of air in pleural cavity chest ... Anatomically, this cavity is formed by the outer membranes of the lungs - pleural sheets. Forms of the disease - open, closed, valve.
Signs of open and closed pneumothorax
Open pneumothorax is a condition in which the pleural cavity communicates directly with the external environment. Inside the cavity, the same pressure is created as in the atmosphere, the air presses on the lung, as a result of which the organ collapses and ceases to function. Gas exchange stops, the level of oxygen in the blood decreases. Open pneumothorax (filling the pleural cavity with blood).
Closed pneumothorax is a relatively mild condition. A certain volume of air enters the pleural cavity, its amount remains unchanged, there is no communication with the external environment. Over time, gases can dissolve on their own, and the lung can resume its anatomical shape.
Ways of air entering the pleural cavity - mechanical open chest trauma, closed damage lung with violation of the integrity of the organ (tissue rupture), emphysema with numerous formations of bulls (air bubbles that burst with a strong cough).
The distinctive symptoms of pneumothorax are sharp, strong pain in the chest with shortness of breath. A person is afraid to take a deep breath, so he breathes often and shallowly. Due to the lack of air, the patient develops a feeling of fear - this is a sign of a closed pneumothorax.
Severe hypoxia (lack of oxygen) leads first to pallor, and then cyanosis (blue discoloration) skinsticky sweat appears especially on the face. Subcutaneous emphysema may develop - an accumulation of gas in the subcutaneous tissue in the chest area.
Open pneumothorax is more dangerous. With a constant increase in the volume of air in the pleural cavity, pressure occurs on the heart and trunk blood vessels... As a result, they are displaced to the side, compressed, blood pressure drops sharply. It is a life-threatening condition that requires urgent medical attention.
Helping patients with closed pneumothorax
 If the amount of air in the pleural cavity is small, the patient has no pronounced symptoms of respiratory failure, the quality of life is not worsened, then this condition does not require specific treatment. Air can be absorbed. But in order to control the process and prevent the aggravation of the situation, the patient must periodically undergo control X-ray examinations.
If the amount of air in the pleural cavity is small, the patient has no pronounced symptoms of respiratory failure, the quality of life is not worsened, then this condition does not require specific treatment. Air can be absorbed. But in order to control the process and prevent the aggravation of the situation, the patient must periodically undergo control X-ray examinations.
With more extensive closed pneumothorax, patients are prescribed drug treatment or operation. The victim is taken to the hospital, to the thoracic or trauma department.
During a chest injury, the person behaves restlessly, when trying to lay him down, resists and takes a sitting position. This is an involuntary action of the body to facilitate breathing. It is difficult for the patient to breathe in a horizontal position. Therefore, he is taken to the hospital only in a half-sitting position.
The first health care before hospitalization is to provide effective pain relief, continuous supply of humidified oxygen, stop falling blood pressure.
In an extremely serious condition of the victim and with severe symptoms of tension pneumothorax (a sharp drop in blood pressure and an acute lack of oxygen, the risk of cardiac arrest), a needle should be punctured immediately in 2-3 intercostal space along the mid-clavicular line. To control the air outlet, a plastic tube from a disposable system is attached to the end of the needle, and a check valve from the finger of a rubber glove is mounted at the end. The tube is placed in a bottle with an antiseptic (furacilin). With correct manipulation, gas bubbles will appear in the solution. The needle is fixed with an adhesive plaster to the skin and in this state the person is transported to the hospital.
Upon admission to the department, emergency care for closed pneumothorax involves draining the pleural cavity through puncture. This manipulation is aimed at simultaneous evacuation of air from the chest.
Bulau drainage

Technique for performing the manipulation:
- Treatment of the puncture site with an antiseptic.
- Local anesthesia with novocaine or lidocaine.
- The puncture is made perpendicular to the chest.
- The needle is inserted slowly. The sign of getting into the cavity is a feeling of sinking and a sharp intense pain.
- A guide wire (thin line) is inserted through the needle, and a drainage catheter is already passed through it with fixation on the skin.
- An aspiration unit is mounted to the tube (water-jet suction, electric).
- Three ampoules are attached, which create the effect of communicating vessels. One container is connected to the drain, into which the contents of the pleural cavity (gas, liquid) will flow, two other ampoules are needed to ensure negative pressure in system.
This method has its drawbacks. Air comes out slowly. If there is fibrin (blood clots) or pus in the cavity, it can clog the tubes. It is also possible for an air cushion to form in the system, which will stop the release of gases. Long-term presence of drainage creates the risk of developing inflammation and phlegmon of the chest.
Helping patients with open pneumothorax
 First aid for open pneumothorax is to prevent air from entering the chest... In order to stop this process, an occlusive dressing is applied to the injury area - an airtight dressing that does not allow air to enter.
First aid for open pneumothorax is to prevent air from entering the chest... In order to stop this process, an occlusive dressing is applied to the injury area - an airtight dressing that does not allow air to enter.
To apply it, you need sterile napkins, a bandage, an airtight material (oilcloth, cellophane), an antiseptic solution.
Rules for effective application of an occlusive dressing:
- Sit the victim facing you, calm down and explain your next steps.
- Wear gloves, conduct a visual inspection of the injury site, determine where air enters the pleural cavity.
- Treat the skin with an antiseptic.
- Put sterile napkins and fix them with adhesive plaster or bandage.
- Cover the injury with oilcloth or plastic wrap from above.
- Finish bandaging.
To prevent the development of painful shock, subcutaneous or intramuscular injections of anesthetic drugs are made. To maintain the heart - adrenaline, atropine. To replenish blood loss, a dropper is connected with special infusion solutions to replenish the BCC (circulating blood volume). To ensure passability respiratory tract the victim is given oxygen therapy (oxygen supply) or artificial ventilation.
The victim is urgently hospitalized in upright position (sitting).
In a hospital setting, first aid for pneumothorax is aimed at removing air from the chest.
 First, a person undergoes primary surgical treatment the wound surface - the edges of the wound are excised, damaged and dead areas are removed, if any foreign bodies, they are removed. This manipulation has three functions:
First, a person undergoes primary surgical treatment the wound surface - the edges of the wound are excised, damaged and dead areas are removed, if any foreign bodies, they are removed. This manipulation has three functions:
- provides aseptic (sterility) of the wound;
- promotes rapid healing;
- prevents the development of infectious complications.
Then they begin to decompress the pleural cavity - the elimination of the air cushion. For this, drainage is carried out according to Bulau.
If the lung is mechanically damaged and its anatomical integrity is violated, the patient undergoes an operation - thoracotomy. This is a surgical opening of the chest for the purpose of a detailed examination of the organs of the chest cavity. If the lung is damaged, the wound is resected or sutured.
Thoracotomy leads to complications in 10% of cases. Patients develop severe pain syndrome requiring the use of narcotic pain medications to relieve pain. IN postoperative period bleeding and suppuration are frequent.
Suturing the wound
 Suturing a lung wound is surgery to restore the integrity and functionality of the lung... For its implementation, there are some difficulties associated with suturing the pulmonary parenchyma. A weak connective tissue framework leads to the fact that after a needle puncture, the wound channel around the suture thread increases in diameter, fills with air and blood. Additional damage is inflicted when trying to tie a knot. The thread cuts into the lung tissue, traumatizing.
Suturing a lung wound is surgery to restore the integrity and functionality of the lung... For its implementation, there are some difficulties associated with suturing the pulmonary parenchyma. A weak connective tissue framework leads to the fact that after a needle puncture, the wound channel around the suture thread increases in diameter, fills with air and blood. Additional damage is inflicted when trying to tie a knot. The thread cuts into the lung tissue, traumatizing.
The purpose of the operation is to ensure the tightness and physiological constancy of the lung... For this, the suture is applied deeply. It is better if the sutures are still applied to the compressed and collapsed organ. To do this, use an atraumatic needle and silk thread.
Traumatic damage to the parenchyma leads to its enlargement and destruction. To stop this process, surgical intervention is required. Lung resection is the excision and removal of part of an organ... Part of the lung is removed in lobes (lobectomy) or segments (segmentectomy). You can delete multiple beats or segments at once.
 If the area of \u200b\u200bthe lesion is small during the injury, a marginal resection is performed. On the outer surface of the lung, the affected tissue is removed.
If the area of \u200b\u200bthe lesion is small during the injury, a marginal resection is performed. On the outer surface of the lung, the affected tissue is removed.
The operation can lead to complications, although they do not occur often. During the surgical intervention there is a risk of severe bleeding associated with a dense circulatory network in the lung parenchyma.
Postoperative complications:
- pneumonia;
- atelectasis - compression of the walls of the organ;
- respiratory and heart failure as a result of the decompensation of the body and its adaptation to new conditions.
Complications of pneumothorax
 Closed and open pneumothorax leads to the development of complications:
Closed and open pneumothorax leads to the development of complications:
- intrapleural bleeding - filling the pleural cavity with blood, followed by the development of collapse;
- subcutaneous emphysema - an accumulation of gases in the subcutaneous tissue of the chest wall;
- serous-fibrous pneumopleuritis - inflammation of the pleura with effusion (fluid accumulation);
- pyothorax - a collection of pus in the chest with high temperature and sharp pains;
- empyema of the pleura - the accumulation of pus in the pleural cavity.
Pneumothorax is a dangerous condition that requires emergency hospitalization and urgent resuscitation measures. If qualified assistance is not provided in a timely manner, pathology can lead to death. Prevention is aimed at reducing injuries (ensuring safety at work, at home, while driving) and timely treatment of diseases of the respiratory system.
Spontaneous pneumothorax (SP) - the flow of air into the pleural cavity between the layers of the pleura in case of damage to the lung, which occurs without previous traumatic effects or other obvious reasons.
Classification of joint ventures depending on its etiology:
1. Primary joint venture -Occurs earlier healthy people, more often against the background of local or widespread bullous emphysema, air cysts or pleural adhesions that do not manifest clinically; the penetration of air into the pleural cavity occurs as a result of a violation of the integrity of the visceral pleura, as it were against the background of complete health and usually at rest.
2. Secondary joint venture -It is a complication of existing diseases of the lungs or pleura: COPD (chronic obstructive bronchitis, pulmonary emphysema, BA), destructive and chronic forms of pulmonary tuberculosis, subpleurally located suppurative processes in the lung (abscess, gangrene, destructive pneumonia), interstitial processes in the lungs, accompanied by the formation of " vicarious "emphysema (silicosis, beryllium disease, silicotuberculosis, sarcoidosis), etc. Development of the secondary joint venture is usually preceded by factors that increase intrapulmonary pressure (lifting of weight, cough, push, etc.)
The clinical picture of the joint venture:
- pain in the corresponding half of the chest - can radiate to the shoulder girdle, upper limb, neck, abdominal cavity; the intensity is determined by the speed and amount of air entering the pleural cavity: with the rapid flow of air, the pain is intense, compared with a blow to the side with a dagger; gradually the pain subsides
- shortness of breath - due to a decrease in the respiratory surface of the lung; the sooner the lung collapses, the more pronounced it is
- dry, paroxysmal or dry cough that aggravates pain and shortness of breath
— general weakness, palpitations, epigastric pain, etc. intermittent and rare complaints
With a tense joint venture patients have increasing shortness of breath, shortness of breath, cyanosis, sweating, tachycardia (140 beats / min and above), hypotension.
Objectively with a small amount of air in the pleural cavity, it is physically difficult to diagnose it, with a significant accumulation of air, there is a limitation of the mobility of the half of the chest, the absence of voice tremor, a box sound on the affected side, the absence of respiratory noise
The main and most informative method for diagnosing joint venture — Chest X-ray:
- signs of the underlying disease, against the background of which a joint venture arose (abscess, tumor, tuberculous focus, cyst, etc.)
- total decline lung tissue in the form of a small shadow at the root of the lung and displacement of the mediastinum with a complete joint venture, partial collapse and the same collapse of all lobes of the lung with partial joint venture (in the presence of pleural adhesions, the collapse of the lung lobes may be uneven)
- a narrow strip of air between the edge of the displaced lung and the inner surface of the chest wall (parietal joint venture when a small amount of air enters the pleural cavity)
- depending on the line of decline, the type of joint venture is determined:
A) closed joint venture - a convex line of decay (because intra-alveolar pressure exceeds intrapleural)
B) open joint venture - a straight line of decay (since intra-alveolar pressure equals with intrapleural pressure)
C) tense joint venture - concave line of decay (since intrapleural pressure exceeds intraalveolar pressure)
The rest of the methods (CT, thoracoscopy) are used mainly to determine the etiology of the joint venture and the choice of treatment method.
Urgent care at SP:
1. If a valvular (stressed) joint venture is suspected - inhalation of humidified oxygen through a mask or nasal catheters + thoracocentesis for health reasons (insertion of a needle with a large hole or a trocar through the 2nd intercostal space along the midclavicular line into the pleural cavity); in the presence of a three-way shut-off valve with a syringe, air aspiration from the pleural cavity is possible (air is aspirated with a syringe partially filled with physical solution, connected through a valve with a needle)
2. Pain relief: keterolac 30 mg (1 ml) intravenously slowly OR 1-2 ml of 50% solution of analgin with 1 ml of 1% solution of diphenhydramine intramuscularly OR with sharp, severe pain 1-2 ml 2 % solution of promedol i / v or i / m
3. In case of collapse - intravenous drip mezaton 1.0 ml 1% or norepinephrine 1.0 ml 0.2% solution per 200 ml physical. solution, in acute heart failure - strophanthin 0.5 ml 0.05% solution IV slowly on physical. solution, with the development of bronchospasm - inhalation of salbutamol 2.5 mg through a nebulizer for 5-10 minutes (if there is no effect, repeat inhalation after 20 minutes)
4. Hospitalization in thoracic surgery or with a strained and bilateral joint venture - in OITAR.
Treatment of joint ventures in hospital:
A) small joint venture (parietal) with minimal symptoms - no treatment required, only observation
B) closed joint venture - pleural punctures with air aspiration (the lung is straightened in 1-2 weeks)
B) open and valve joint venture - underwater drainage according to Bulau (after 2-4 days the open one should become closed, it is effective in 90% of cases); if, 5 days after drainage, the lung does not expand and air seepage continues, the treatment is surgical (thoracotomy with suturing of bullae and scarification of the pleura), and if it is ineffective (recurrent joint venture) or impossibility, pleurodesis (introduction of sclerosing substances into the pleural cavity - tetracycline, talc, cytostitics)
Pneumothorax is a pathology in which air is concentrated in the pleural cavity, penetrating there from damaged lungs or through existing defects in the chest. This acute condition threatens the patient's life, it occurs in our time quite often and requires urgent medical attention.
The term "pneumothorax" literally means "air in the chest." Pneumothorax - stagnation of air masses and gaseous substances between the layers of the pleural cavity. Exist various forms diseases, each of which has its own characteristics and methods of treatment.
Classification
Depending on the causative factors, pneumothorax is divided into:
- Post-traumatic - is a consequence of traumatic injuries of the chest.
- Spontaneous - develops independently in healthy people or with a history of chronic pulmonary pathology: abscess, gangrene, emphysema, or.
- Iatrogenic or artificial pneumothorax is the result of medical procedures.
Pathogenetically, the disease is classified into forms:
- Closed - the most light variety pneumothorax, in which there is no communication with the external environment.
- Open - characterized by depressurization of the respiratory system. Air enters the pleural cavity during inhalation and is removed during exhalation, without accumulating in the body.

Open pneumothorax
- Valve - air enters the pleural cavity through the wound and does not leave it. It is concentrated between the pleural sheets, and intrapleural pressure builds up rapidly. Further progression of the pathology ends with damage to the neurovascular bundles and compression of the second lung. Valvular pneumothorax becomes tense - the most dangerous species pathology leading to the death of the patient.

Tension pneumothorax
By localization, pneumothorax is one-sided (left- or right-sided) and bilateral.
By the degree of lung collapse:
- Partial or limited collapse - the lung falls by 1/3,
- Subtotal collapse - the lung falls by ½,
- Total collapse - the lung collapses by more than ½ or is completely compressed by air.
If, in addition to air, blood is contained in the pleural cavity, then they speak of hemopneumothorax, if pus - pyopneumothorax.
Etiology
Risk factors for spontaneous pneumothorax are:
The causes of pneumothorax are divided into 2 large groups:
- The influence of mechanical factors - trauma, injury, improperly performed medical and diagnostic procedures, artificial pneumothorax.
- Specific and nonspecific pulmonary pathology - tuberculous infection, abscess and gangrene of the lung, rupture of the esophagus.
Primary spontaneous pneumothorax occurs after physical exertion, sudden movements, coughing, or at rest, often during sleep.
Symptoms
The disease begins suddenly. First shortness of breath appears, breathing becomes shallow and rapid. Then pain syndrome develops: there is a sharp pain in the chest, which is activated by breathing and movement, radiating to upper limbs... Shortness of breath and pain are often accompanied by bouts of dry cough.
The skin becomes pale, sweaty and clammy, and the heart rate increases. As carbon dioxide accumulates in the blood, cyanosis develops - cyanosis of the skin. To at least slightly reduce pain, patients take a forced posture - half-sitting or lying down. Patients feel weakness, fear, panic. Their heart rate increases and blood pressure drops. The mobility of the chest from the affected side is limited and lags behind in the act of breathing, and with the healthy side it is enhanced. Intercostal spaces are smoothed.
The clinical picture of the disease in children practically does not differ from that in adults, but is characterized by a rapid increase in the symptoms of pneumothorax and the appearance of seizures. The younger the child, the heavier they are.
Complications
The prognosis for pneumothorax is favorable. The air in the pleural cavity is absorbed within 3-5 weeks, and complete recovery occurs.
Pneumothorax is often complicated by the development of exudative inflammation of the pleura with the accumulation of hemorrhagic and serous-fibrinous effusion.
The dangerous consequences of pneumothorax are: adhesions that interfere with lung expansion; bleeding into the pleural cavity from the affected vessel; hemothorax; pyothorax; sepsis; stiff lung; purulent fusion of the pleura.
Long-term current pneumothorax often ends with the replacement of connective tissue of the lung tissue, wrinkling of the lung, loss of elasticity, the development of pulmonary and heart failure, and death.
Diagnostics
Diagnosis of pneumothorax is based on data obtained during examination and examination of the patient. Percussion reveals a boxy or tympanic sound, spreading to the lower ribs, displacement or expansion of the boundaries of cardiac dullness. Weakening or absence of voice tremor is determined by palpation. Breathing is weakened or not heard.
X-ray examination allows you to detect the zone of enlightenment and displacement of the mediastinal organs, there is no pulmonary pattern. A more detailed image can be obtained using computed tomography... Additional diagnostic methods are: pleural puncture with manometry, videothoracoscopy, blood gas analysis, electrocardiography.
With hemopneumothorax and pyopneumothorax, a diagnostic puncture is performed to determine the cellular composition and the presence of pathogenic microbes.
Treatment
Pneumothorax is a pathological process that poses a threat to the patient's life. Patients with pneumothorax are shown hospitalization in a surgical hospital. Treatment of the disease should begin before the arrival of the ambulance team. The patient should be helped - to calm down, restrict the mobility of the chest and provide sufficient oxygen. The ambulance doctor examines the patient, feels the chest, prescribes the necessary diagnostic tests.

Drainage of the pleural cavity
If a large amount of air accumulates in the pleural cavity, it drained using a Bobrov apparatus or an electric aspirator. This is a simple medical procedure that does not require special preparation of the patient.
The procedure is performed under local anesthesia. The patient is seated and the place of installation of the drainage "Novocain" is injected. Then a trocar is inserted, with the help of which the drainage is established. It is fixed to the skin and attached to Bobrov's jar. If this method of drainage becomes ineffective, proceed to active aspiration. The drain is connected to an electric pump and drained until the lung is fully expanded, confirmed by X-ray.
Surgery
If active aspiration does not allow to stop pneumothorax or if it recurs, go to surgical treatment - carrying out thoracotomy.
 The pleural cavity is opened, the cause of the pathology is eliminated, and then the existing defect in the lung tissue is sutured, bleeding is stopped and the wound is sutured layer by layer, leaving a drainage tube.
The pleural cavity is opened, the cause of the pathology is eliminated, and then the existing defect in the lung tissue is sutured, bleeding is stopped and the wound is sutured layer by layer, leaving a drainage tube.
Indications for thoracotomy are:
- Ineffectiveness of pleural drainage,
- Bilateral spontaneous pneumothorax,
- Hemopneumothorax,
- Relapses of pathology caused by bullous emphysema.
Prevention
- Timely diagnosis and treatment of respiratory diseases,
- Regular fluorographic examination of the lungs,
- Surgical removal of the source of the disease,
- Anti-smoking,
- Respiratory gymnastics in the open air.
Persons with a history of pneumothorax should avoid excessive physical activity, refrain from flying, diving, parachuting for a month.
Pneumothorax is a serious life-threatening illness that requires medical attention. The sooner a patient with pneumothorax turns to medical institution, the more chances he has for recovery.
Video: pneumothorax, medical animation
Pneumothorax is a pathological accumulation of air or other gases in the pleural cavity, leading to a violation of the ventilation function of the lungs and gas exchange during breathing.
Pneumothorax leads to compression of the lungs and oxygen deficiency (hypoxia), metabolic disorders and respiratory failure.
Kinds
Pneumothorax is basically two different types depending on the origin and communication with the external environment:
- closed, when the tightness of the chest is preserved, and air or gases enter through the defect in that part of the pleura that communicates with the lungs. In this case, excess air or gas enters the pleural cavity from the respiratory tract.
- open, when gas or air enters the pleural cavity from the external environment through defects in the chest - injuries, while there is a depressurization of the respiratory system.
According to the mechanisms of development, there are:
- open pneumothorax, when air enters the pleural cavity during inhalation and leaves it during exhalation,
- closed (tense) acts on the valve mechanism. On inhalation, air enters the pleural cavity, and on exhalation, the tissues are compressed, preventing air from coming back, as a result, the pressure in the pleural cavity slowly but surely increases.
Also distinguish:
- spontaneous pneumothorax that occurs without any previous disease, or a disease that was latent,
- secondary pneumothorax arising as a complication of pulmonary or extrapulmonary pathology,
- artificial pneumothorax, which is created by doctors when certain manipulations are necessary.
The reasons
The main causes of pneumothorax include several groups:
- trauma, mechanical damage chest and closed lungs with fractures of the ribs and damage to the lungs,
- penetrating wounds of the chest (gunshot, stab),
- complication of diagnostic or treatment measures (when placing a catheter, puncture, nerve blockade),
- the imposition of an artificial pneumothorax during diagnosis or treatment.
Another group of causes is lesions and diseases of the chest cavity - ruptures of bullae and cysts in emphysema of the lungs, breakouts of abscesses, rupture of the esophagus, tuberculous process, tumor processes with melting of the pleura.
Pneumothorax usually occurs on one side, but it can also be bilateral, usually large injuries or severe damage to the lungs and pleura.
Signs of pneumothorax
The manifestations of the clinic of pneumothorax will depend on what is the cause of it and how much the lung is compressed or both of them.
Symptoms of open pneumothorax
With open pneumothorax, patients usually lie on the injured side of the chest, clutching the wounds with their hands. At the same time, a noisy suction of air into the chest cavity is strongly audible, while foamed blood oozes at the site of the wound, when viewed, the chest is asymmetric, since the affected lung is less involved in breathing.
Symptoms of spontaneous pneumothorax
Spontaneous pneumothorax occurs acutely, usually preceded by an attack severe cough or heavy physical exertion, sometimes even a deep breath is sufficient.
The typical onset of pneumothorax is severe stabbing pain in the area of \u200b\u200bthe affected lung with a return to the sternum or neck and arm.
When coughing or breathing deeply, the pain is stronger, movements provoke increased pain, which can cause fear of death and panic.
With pain syndrome, shortness of breath also occurs, depending on the degree of compression of the lungs, there may be signs of respiratory failure, blueness of the face or sharp pallor, dry cough, which is suppressed by the patient due to pain.
As the symptoms increase, the pain subsides, the shortness of breath becomes weaker, and soreness occurs only with deep breathing or moving the patient. Subcutaneous swelling (emphysema) may occur in the wound or in the neck and face, which gives a crunching sensation when pressure is applied to the swollen areas.
When listening to the lungs, breathing will be sharply weakened, or the lung does not breathe at all. Signs of pneumothorax begin to appear when the lung volume decreases by 30-40%, as the process develops, the pleura becomes inflamed, and after a few hours, edema and fibrin deposits on the pleura develop, which leads to adhesions between the lung and pleura, which will then interfere with the normal expansion of the lung during treatment.
Diagnostics
Diagnostics in case of suspected pneumothorax is based on examination and listening to the lungs with the identification of zones of lack of breathing from below.
In addition, suspicions are given by typical signs on the part of the patient - forced position of the body, decreased pressure, indications of chest trauma, breathing disorders.
The final verdict is made by an X-ray, which shows a compressed lung and an air zone in the pleural cavity, and the displacement of organs away from the lesion is also visible.
A pleural puncture with the production of gas or air will help establish the diagnosis, while the pressure in the cavity will be zero.
Treatment of pneumothorax
Pneumothorax is a condition requiring emergency care, which will be provided in a hospital. Pneumothorax is treated by surgeons and pulmonologists. Open pneumothorax requires an airtight dressing, valvular pneumothorax requires urgent puncture with removal of air and further surgery to remove the suction valve.
In the future, treatment in a hospital will depend on the causes of pneumothorax - this is the removal of air, restoration normal pressure inside the pleura, and suturing wounds, removing fragments of ribs, lung surgery, etc.
In order to suppress the development of pneumothorax again, the procedure of pleurodesis is carried out - the creation of artificial adhesions in the pleura with a completely expanded lung.
Prognosis after pneumothorax
Treatment and rehabilitation after pneumothorax last from 1-2 weeks to several months, it all depends on the cause.
The prognosis for pneumothorax depends on the degree of damage and the rate of development of respiratory failure. In case of injury and trauma, it can be unfavorable.
Open pneumothorax - This is the accumulation of air in the pleural cavity due to an open wound channel in the chest. As a result, the difference between the pressure in the external environment and in the pleural cavity is smoothed out, and the alveoli of the lungs stick together and cease to perform the function of gas exchange.
Trauma provokes constant pressure drops, displacement of the heart, bronchi, lungs occurs, and also kinks and compression of blood vessels are observed circulatory system... These processes, together with the irritating effect of air on the pleura, provoke the development of paradoxical respiration syndrome and cardiopulmonary disorders, which is manifested in a severe shock state of the victims.
In contact with
Classmates
Reasons for education

Open pneumothorax can be a complication of some unsuccessful medical procedures. These include:
- Subclavian vein catheterization;
- sampling of pleural punctate;
- intercostal nerve block.
During these procedures, there is a certain risk of a needle puncture of the lung.
But the main reasons are:
- penetrating and gunshot wounds sternum;
- an open fracture of the ribs, fragments of which damage the lungs.
Symptoms (signs) of open pneumothorax
- Open wound of the chest region, combined with pale skin and cyanosis;
- the wounded person lies on the injured side, breathes with a characteristic "suction" sound and tries to hold the wound with his palm;
- respiratory movements are frequent, shallow. The pressure is below normal. Pulse of weak filling, frequent;
- bloody foamy discharge from the wound;
- the rib cage rises asymmetrically.
Kinds
Open pneumothorax is divided into:
- Full;
- partial;
- bilateral;
- unilateral.
When partial pneumothorax the volume of air in the pleural cavity is small. Therefore, the lung does not completely collapse, and continues to function in a limited volume.
The most dangerous condition for the victim is bilateral complete pneumothorax... At the same time, the respiratory functions are so depressed that the absence necessary measures leads to the death of the victim.
Diagnostics

Most often, a single visual examination is sufficient to diagnose open pneumothorax. Additional methods include:
- Auscultatory - breathing is weakened when listening;
- percussion - percussion on the damaged side of the tympanitis injury;
- x-ray examination - X-ray in the pleural cavity can reveal an accumulation of gas, a compressed lung and displacement of the mediastinal organs.
Providing emergency care
The first measures are to call the ambulance team and apply to the wound hermetic occlusive dressing in order to prevent the penetration of air from the outside. The victim can be given pain relievers: promedol or analgin and urgently transport to a medical facility.
An open pneumothorax is a medical emergency.
Application of an occlusive dressing for open pneumothorax
Treat the skin around the wound with antiseptics and petroleum jelly. The wound itself is covered with sterile cotton-gauze pads, a sealed package from the emergency package is placed on top (with the clean side to the wound), or plastic wrap or any glued material. Then compress paper, a layer of gauze and everything is wrapped with bandages or sealed with a plaster. In the absence of a sealed film, a thick bandage of several layers of bandage and cotton wool is applied.
 Smoking, an unhealthy lifestyle can lead to serious changes in the lungs. You are risking your health and should definitely know.
Smoking, an unhealthy lifestyle can lead to serious changes in the lungs. You are risking your health and should definitely know.
Early diagnosis pneumonia is the main factor effective treatment... on the methods of diagnosing this disease.
In the event that there is no material for dressing, the wound is simply tightly closed with plastic wrap or cellophane (it is advisable to treat them with alcohol or any antiseptic), and fixed before the arrival of the medical team.
First aid
Medical measures are as follows:
- Hermetic wound suturing;
- pleural puncture;
- air removal.
Air is removed to restore the required pressure difference between the chest cavity and the external environment.
According to indications, artificial lung ventilation is performed.
Forecast
With timely assistance, the prognosis is favorable. However, 50% of victims subsequently develop complications such as: pneumopleuritis, pleural empyema, intrapleural bleeding. Also, the transferred open pneumothorax can contribute to the formation of connective tissue strands that prevent the straightening of the lung.
You can learn about the purpose and rules of applying an occlusive dressing for open pneumothorax from the following video.
In contact with