Conn's syndrome (primary hyperaldosteronism). Primary hyperaldosteronism (Connes syndrome) Assessment of the aldosterone-renin ratio
Conn's syndrome is a disease endocrine system, which is characterized by a large amount of aldosterone production. In medicine, it is referred to as primary aldosteronism. This ailment can be called a consequence of the main disease, which, as it progresses, causes complications. The main diseases include adrenal tumor, adrenal cancer, pituitary neoplasm, adenoma and carcinoma.
General information
Aldosteronism is divided into primary and secondary. Both are due to the overproduction of the hormone aldosterone, which is responsible for the retention of sodium in the body and the excretion of potassium by the kidneys. This hormone is also called the adrenal cortex hormone and mineralocorticoid. The most common and severe companion of this disease is arterial hypertension. Primary and secondary aldosteronism are not two stages of one disease, but two completely different diseases. They also differ in the causes of appearance, the effect on the body and, accordingly, in the method of treatment.
Primary (Connes' syndrome) aldosteronism
Opened Mr. Conn in 1955. Women are 3 times more likely to suffer from aldosteronism. At risk is the fair sex at the age of 25-45 years. Primary aldosteronism occurs due to neoplasms of the adrenal cortex (unilateral adenoma). Much less often, the cause is adrenal hyperplasia or cancer. With increased production of aldosterone, the amount of sodium in the kidneys increases, and potassium, in turn, decreases.
The study is carried out by a pathologist who diagnoses a tumor of the adrenal cortex. It can be single or multiple and affect one or both of the adrenal glands. In more than 95% of cases, the tumor is benign. Also, as a study, doctors often prescribe an enzyme immunoassay, where venous blood is used as a biomaterial. An ELISA is prescribed to determine the amount of aldosterone in the body and for screening for primary hyperaldosteronism.
 Conn's syndrome occurs with adrenal pathology, tumor neoplasms.
Conn's syndrome occurs with adrenal pathology, tumor neoplasms. The indications for the study are most often high blood pressure, which does not return to normal with therapeutic manipulations, suspicion of the development of renal failure. To donate blood, you need to properly prepare. First, limit your carbohydrate-rich foods for 2-4 weeks. Also for this period, exclude diuretics, estrogens, oral contraceptives, steroids. For 1 week, stop therapy with renin inhibitors, remove for 3 days, in extreme cases - limit, mental and physical overstrain. Do not smoke three hours before the procedure. Having the results on hand, taking into account the amount of hormones renin, aldosterone and cortisone, the attending physician will be able to correctly diagnose and prescribe effective drug treatment.
Secondary compensatory (symptomatic)
Unlike primary aldosteronism, secondary aldosteronism is triggered not by diseases associated with the adrenal glands, but by problems with the liver, heart and kidneys. That is, it acts as a complication of some serious diseases. At risk are patients with a diagnosis of:
- adrenal cancer;
- a number of heart diseases;
- abnormalities in work thyroid gland, intestines;
- idiopathic hyperaldosteronism;
- adenoma of the adrenal cortex.
Also, a tendency to bleeding, prolonged exposure to medications should be added to the list. But this does not mean that all patients who suffer from these ailments will add the diagnosis of "secondary aldosteronism" to their medical history, they just should be more attentive to their health.
Disease symptoms
 Persistent arterial hypertension is a characteristic symptom of Conn's syndrome.
Persistent arterial hypertension is a characteristic symptom of Conn's syndrome. Primary and secondary aldosteronism are associated with the following symptoms:
- puffiness that appears due to fluid retention in the body;
- weakening of muscle strength, fatigue;
- frequent urge to use the toilet, especially at night (pollakiuria);
- hypertension (increased blood pressure);
- thirst;
- vision problems;
- bad state of health, headache;
- muscle paralysis for short periods of time, numbness of body parts, slight tingling;
- an increase in the size of the ventricles of the heart;
- rapid weight gain - more than 1 kg per day.
The evacuation of potassium contributes to the appearance of muscle weakness, paresisia, sometimes muscle paralysis and many other renal diseases. The symptoms of aldosteronism are quite dangerous, but the consequences are no less dangerous. Therefore, do not hesitate, you need to consult a doctor for help as soon as possible.
Complications and consequences
Primary aldosteronism, if symptoms are ignored and therapy is abandoned, leads to a number of complications. First of all, the heart begins to suffer (ischemia), heart failure, intracranial bleeding develops. In rare cases, the patient has a stroke. Since the amount of potassium in the body decreases, hypokalemia develops, which provokes arrhythmia, which, in turn, can be fatal. Secondary hyperaldosteronism itself is a complication of other serious ailments.
Diagnosis and differential diagnosis
 Urine and blood tests are prescribed for the correct and accurate diagnosis of the disease.
Urine and blood tests are prescribed for the correct and accurate diagnosis of the disease. If the attending physician is suspected of aldosteronism, a number of studies and tests are prescribed in order to confirm or refute the alleged diagnosis, as well as for correct further drug therapy. First of all, urine and blood tests are performed. The laboratory establishes or refutes the presence of polyuria or analyzes its urine density. The concentration of aldosterone, cortisol and renin is studied in the blood. With primary hyperaldosteronism, there is little renin, the amount of cortisol is normal, and the amount of aldosterone is high. For secondary aldosteronism, a somewhat different situation is inherent, the presence of renin should be essential. Ultrasound is often used for more accurate results. Less commonly, MRI and CT of the adrenal glands. Additionally, the patient should be examined by a cardiologist, ophthalmologist, nephrologist.
Treatment of aldosteronism
Treatment of primary or secondary aldosteronism should be comprehensive and include more than drug therapyand and proper nutrition, in some cases - operational surgical intervention. The main goal of curing Connes syndrome is to prevent complications after The diet for Crohn's disease depends on the severity of the symptoms of the disease.
In parallel, you should follow a diet. It is based on an increase in potassium-containing products and additional potassium-containing preparations. Eliminate or limit salt intake. Potassium-rich foods include:
- dried fruits (raisins, dried apricots, prunes);
- fresh fruits (grapes, melon, apricots, plums, apples, banana);
- fresh vegetables (tomato, potatoes, garlic, pumpkin);
- greens;
- meat;
- nuts;
- black tea.
Definition of the concept
In 1955, Cohn described a syndrome characterized by arterial hypertension and a decrease in serum potassium levels, the development of which is associated with aldosteroma (an adenoma of the adrenal cortex that secretes aldosterone).
Primary hyperaldosteronism more common in adults, more often women are ill (ratio 3: 1) at the age of 30-40 years. Among children, the incidence of the disease in girls and boys is the same.
Causes of the disease
1. Aldosteromas (Cohn's syndrome)
2. Bilateral adrenal hyperplasia or multiple adenomatosis of the adrenal cortex (15%):
a) idiopathic hyperaldosteronism (overproduction of aldosterone is not suppressed);
3. Aldosterone-producing adenoma, completely suppressed by glucocorticoids.
4. Carcinoma of the adrenal cortex.
5. Extra-adrenal hyperaldosteronism
Mechanisms of the onset and development of the disease (pathogenesis)
1. Aldosteromas (Cohn's syndrome) - aldosterone-producing adrenal tumor (70% of cases of primary hyperaldosteronism). Aldosterone-producing adenoma of the adrenal cortex is usually unilateral, no more than 4 cm in size. Multiple and bilateral adenomas are extremely rare. Adrenal cancer as a cause of aldosteronism is also rare - 0.7-1.2%. In the presence of an adenoma, aldosterone biosynthesis does not depend on ACTH secretion.
2. Bilateral adrenal hyperplasia (30% of cases) or multiple adenomatosis of the adrenal cortex (15%):
a) idiopathic hyperaldosteronism (overproduction of aldosterone, not suppressed);
b) undefined hyperaldosteronism (overproduction of aldosterone, selectively suppressed);
c) hyperaldosteronism, completely suppressed by glucocorticoids.
3. Aldosterone-producing adenoma, is completely suppressed by glucocorticoids.
4. Carcinoma of the adrenal cortex.
A relatively rare cause of primary aldosteronism is a malignant tumor of the adrenal cortex.
5. Extra-adrenal hyperaldosteronism (tumor of the ovaries, intestines, thyroid gland).
Malignant tumors account for 2-6% of all cases.
The clinical picture of the disease (symptoms and syndromes)
1. Arterial hypertension. Persistent arterial hypertension is sometimes accompanied by severe headaches in the forehead. Hypertension is stable, but paroxysms are possible. Malignant hypertension observed very rarely.
Hypertension does not respond to orthostatic load (renin-dependent reaction), resistant to the Valsalva maneuver (blood pressure does not increase during the test, unlike other types of hypertension).
BP is corrected with spironolactone (400 mg / day for 10-15 days), as is hypokalemia.
2. "Kaliypenichesky kidney"
In almost all cases, primary aldosteronism is accompanied by hypokalemia due to excessive loss of potassium by the kidneys under the influence of aldosterone. Potassium deficiency causes the formation of a "caliopenic kidney". The epithelium of the distal renal tubules is affected, in combination with general hypokalemic alkalosis, leading to a violation of the mechanisms of oxidation and urine concentration.
In the initial stages of the disease, renal impairment may be minor.
1) Polyuria, mainly nocturnal, reaches 4 liters per day, nocturia (70% of patients). Polyuria in primary hyperaldosteronism is not suppressed by vasopressin drugs, and does not decrease with fluid intake restriction.
2) Typical hypoisostenuria - 1008-1012.
3) Transient, moderate proteinuria is possible.
4) The urine reaction is often alkaline, which increases the incidence of concomitant pyelitis and pyelonephritis.
Thirst and compensatory polydipsia develop as a reaction to polyuria. Polydipsia and polyuria at night, along with neuromuscular manifestations (weakness, paresthesias, myoplegia attacks), are mandatory components of the hypokalemic syndrome. Polydipsia has a central origin (hypokalemia stimulates the center of thirst) and reflex genesis (due to the accumulation of sodium in cells).
Swelling is not typical - only in 3% of patients with concomitant kidney damage or circulatory failure. Polyuria, accumulation of sodium in cells does not contribute to fluid retention in the interstitial space.
3. Muscle damage. Muscle weakness, pseudoparalysis, periodic seizures of varying intensity, tetany is observed, overt or latent. Twitching of facial muscles, positive symptoms of Khvostek and Trusso are possible. Increased electrical potential in the rectum. Characteristic paresthesias in various muscle groups.
4. Changes in the central and peripheral nervous system
General weakness manifests itself in 20% of patients. Headaches are observed in 50% of patients, are intense - caused by an increase in blood pressure and hyperhydration of the brain.
5. Violation of carbohydrate metabolism.
Hypokalemia suppresses insulin secretion, promotes the development of reduced carbohydrate tolerance (60% of patients).
Diagnosis of the disease
1. Hypokalemia
Increased urinary potassium excretion (normally 30 mmol / l).
2. Hypernatremia
3. Hyperosmolarity
Specific stable hypervolemia and high plasma osmolarity. An increase in intravascular volume of 20-75% does not change with the introduction of saline or albumin.
Alkalosis is present in 50% of patients - blood pH reaches 7.60. Increased blood bicarbonate content up to 30-50 mmol / l. Alkalosis is combined with a compensatory decrease in the level of chlorine in the blood. The changes are enhanced by the use of salt, and are eliminated by spironolactone.
4. Violation of hormonal levels
The level of aldosterone in the blood is often increased at a rate of 2-16 ng / 100 ml to 50 ng / 100 ml. Blood sampling should be carried out with the patient in a horizontal position. Increased blood levels of aldosterone metabolites. Changes in the daily profile of aldosterone secretion: determination of the level of aldosterone in the blood serum at 8 am and at 12 noon. With aldosteroma, the content of aldosterone in the blood at 12 noon is lower than at 8 a.m., whereas with small- or large-nodular hyperplasia, the concentration of aldosterone during these periods hardly changes or slightly higher at 8 a.m.
Increased urinary excretion of aldosterone.
Reduced unstimulated plasma renin activity is a cardinal symptom of primary hyperaldosteronism. Renin secretion is suppressed by hypervolemia and hyperosmolarity. In healthy people, the content of renin in the blood in a horizontal position is 0.2-2.7 ng / ml / hour.
The criterion for the diagnosis of the syndrome of primary hyperaldosteronism is a combination of decreased plasma renin activity with hyperaldosteronemia. Differential diagnostic criterion from secondary hyperaldosteronism in renovascular hypertension, chronic renal failure, renin-forming kidney tumor, malignant arterial hypertension, when both the level of renin and aldosterone are increased.
5. Functional tests
1. Load with sodium 10 g / day for 3-5 days. In practically healthy individuals with normal regulation of aldosterone secretion, the serum potassium level will remain unchanged. With primary aldosteronism, the content of potassium in the blood serum decreases to 3-3.5 mmol / l, the excretion of potassium in the urine sharply increases, the patient's condition worsens (severe muscle weakness, heart rhythm disturbances).
2. 3-day diet low (20 mEq / day) sodium - the level of renin remains unchanged, the level of aldosterone may even decrease.
3. Test with furosemide (lasix). Before the test, the patient should be on a diet with a normal sodium chloride content (about 6 g per day), not receive any antihypertensive drugs for a week, and not take diuretics for 3 weeks. When conducting a sample, the patient takes 80 mg of furosemide orally and for 3 hours is in upright position (walks). After 3 hours, blood is taken to determine the level of renin and aldosterone. In primary aldosteronism, there is a significant increase in aldosterone levels and a decrease in the concentration of renin in the blood plasma.
4. Test with kapoten (captopril). In the morning, blood is taken from the patient to determine the content of aldosterone and renin in plasma. Then the patient takes 25 mg of capoten orally and for 2 hours is in sitting position, after which blood is taken from him again to determine the content of aldosterone and renin. In patients with essential hypertension, as well as in healthy people, there is a decrease in the level of aldosterone due to inhibition of the conversion of angiotensin I to angiotensin II. In patients with primary aldosteronism, the concentration of aldosterone is increased, the ratio of aldosterone / renin activity is more than 50.
5. Spironolactone test. The patient is on a diet with a normal sodium chloride content (6 g per day) and for 3 days receives aldosterone antagonist aldactone (veroshpiron) 100 mg 4 times a day. On the 4th day, the potassium content is determined in the blood serum, and an increase in its blood level by more than 1 mmol / l compared to the initial level is confirmation of the development of hypokalemia due to an excess of aldosterone. The level of aldosterone and renin in the blood remains unchanged. Arterial hypertension is eliminated.
6. Test with non-aldosterone mineralocorticoids. The patient takes 400 μg of fluorocortisol acetate for 3 days or 10 mg of deoxycorticosterone acetate for 12 hours. The level of aldosterone in the blood serum and the excretion of its metabolites in the urine during primary aldosteronism does not change, while in secondary hyperaldosteronism, it decreases significantly. In some cases, there is a slight decrease in the level of aldosterone in the blood also with aldosteroma.
7. Test with DOX. Doxa is prescribed at 10-20 mg / day for 3 days. In patients with secondary hyperaldosteronism, the level of aldosterone decreases, in patients with Cohn's syndrome - not. Glucocorticosteroid and androgen levels are normal.
8. Orthostatic test (walking for 4 hours). Unlike healthy people, aldosterone levels are paradoxically reduced.
9. Topical diagnosis of adrenal lesions. Adenomas-aldosteromas are small, in 80% of patients less than 3 cm in diameter, more often located in the left adrenal gland.
10. Computed tomography is the most informative study with high sensitivity. In 90% of patients, tumors with a diameter of 5-10 mm are detected.
11. Scanning of the adrenal glands with I-131-iodine-cholesterol against the background of inhibition of glucocorticoid function by dexamethasone (0.5 mg every 4 hours for 4 days). The asymmetry of the adrenal glands is characteristic. Sensitivity - 85%.
12. Catheterization of the adrenal veins with bilateral selective blood sampling and determination of the level of aldosterone in them. The sensitivity of the study increases after preliminary stimulation of the adenoma with synthetic ACTH - the production of aldosterone on the side of the tumor sharply increases. The sensitivity of the study is 90%.
13. X-ray contrast venography of the adrenal glands - the sensitivity of the method is 60%: the vascularization of the tumor is insignificant, the size is small.
14. Echography of the adrenal glands.
15. Suprareno-radiography in conditions of pneumoretroperitonium, combined with or without intravenous urography. The method is informative only when large tumors, often gives false negative results. The small size of the aldosteromas located inside rarely change the contours of the adrenal glands.
Differential diagnosis
1. Secondary aldosteronism (hyperreninemic hyperaldosteronism) - conditions in which advanced education aldosterone is associated with long-term stimulation of its secretion by angiotensin II. For secondary aldosteronism, an increase in the level of renin, angiotensin and aldosterone in blood plasma is characteristic. The activation of the renin-angiotensin system occurs due to a decrease in the effective blood volume with a simultaneous increase in the negative balance of sodium chloride. It develops in nephrotic syndrome, cirrhosis of the liver in combination with ascites, idiopathic edema, which are often found in premenopausal women, congestive heart failure, renal tubular acidosis.
2. Barter's syndrome: hyperplasia and hypertrophy of the juxtaglomerular apparatus of the kidneys with hyperaldosteronism. The excessive loss of potassium in this syndrome is associated with changes in the ascending renal tubules and a primary defect in chloride transport. It is characterized by dwarfism, mental retardation, the presence of hypokalemic alkalosis with normal blood pressure.
3. Tumors producing renin (primary reninism), including Wilms' tumors (nephroblastoma) - secondary aldosteronism occurs with arterial hypertension... Malignant hypertension with renal and retinal vascular damage is often combined with increased renin secretion and secondary aldosteronism. Increased renin formation is associated with the development of necrotizing renal arteriolitis. After nephrectomy, both hyperaldosteronism and hypertension disappear.
4. Long-term use of thiazide diuretics in arterial hypertension causes secondary aldosteronism. Therefore, the determination of the level of renin and aldosterone in the blood plasma should be carried out only 3 weeks or later after the discontinuation of diuretics.
5. Long-term use of contraceptives containing estrogen leads to the development of arterial hypertension, an increase in the level of renin in the blood plasma and secondary aldosteronism. The increase in renin formation is associated with the direct effect of estrogens on the liver parenchyma and an increase in the synthesis of a protein substrate - angiotensinogen.
6. Pseudomineralocorticoid hypertensive syndrome is accompanied by arterial hypertension, a decrease in the content of renin and aldosterone in the blood plasma. It develops with excessive use of glycyrlysinic acid preparations (glycyram, sodium glycyrinate) contained in the rhizomes of Ural licorice or licorice naked.
7. Liddle's syndrome is a hereditary disease, accompanied by increased sodium reabsorption in the renal tubules with the subsequent development of arterial hypertension, a decrease in the content of potassium, renin and aldosterone in the blood.
8. Reception or excessive formation of deoxycorticosterone in the body leads to sodium retention, excessive potassium excretion and hypertension. With a congenital disorder of the biosynthesis of cortisol distal to 21-hydroxylase, namely, with a deficiency of 17a-hydroxylase and 11b-hydroxylase, an excessive formation of deoxycorticosterone occurs with the development of a corresponding clinical picture.
9. Hypertonic disease with a low content of renin in the blood plasma (nizkoreninovy \u200b\u200barterial hypertension) is 20-25% of all patients suffering from this disease. The use of steroidogenesis inhibitors in hypertensive patients with low renin content led to normalization blood pressure, while in hypertensive patients with normal renin levels, such treatment was ineffective. The normalization of blood pressure was observed in such patients after bilateral total adrenalectomy. It is possible that hypertension with a low renin content is a hypertensive syndrome that develops due to an excess of secretion of yet unidentified mineralocorticoids.
 Hyperaldosteronism is a syndrome caused by hypersecretion of aldosterone (mineralocorticoid hormone of the adrenal cortex), accompanied by arterial hypertension and severe electrolyte disturbances. It is customary to highlight the primary and.
Hyperaldosteronism is a syndrome caused by hypersecretion of aldosterone (mineralocorticoid hormone of the adrenal cortex), accompanied by arterial hypertension and severe electrolyte disturbances. It is customary to highlight the primary and.
Primary hyperaldosteronism is a consequence of the primary excess production of aldosterone directly in the glomerular layer of the adrenal cortex.
In secondary hyperaldosteronism, stimulation of the production of excess aldosterone occurs due to the influence of pathological factors outside the adrenal glands. In addition, a group of diseases is distinguished, which are characterized by similar symptoms, not accompanied by an increased level of aldosterone (syndromes that mimic hyperaldosteronism).
Primary hyperaldosteronism, first described by Konn in 1956, is in most cases the result of an autonomous solitary aldosterone-producing adrenal adenoma ( connes syndrome), less often - macronodular or micronodular bilateral hyperplasia (idiopathic hyperaldosteronism) or adrenal cancer. In most cases, a unilateral adrenal adenoma is detected, usually small in size (up to 3 cm in diameter), occurring with equal frequency on both sides.
Etiology and pathogenesis
The disease is more common in women (2 times more often than in men), usually between the ages of 30 and 50. Since the main symptom of hyperaldosteronism is arterial hypertension, of fundamental importance is the fact that primary hyperaldosteronism is detected in approximately 1% of the general population of patients with arterial hypertension. The cause of the disease is unknown. It should be remembered that hyperaldosteronism caused by hyperplasia of the glomerular zone of the adrenal cortex is characterized by preservation of sensitivity to stimulation by angiotensin II.
In addition, familial hyperaldosteronism is isolated, suppressed by glucocorticoids and with preserved sensitivity to pituitary ACTH (familial type I hyperaldosteronism), which develops as a result of the formation of a defective enzyme during crossing over of the 11-β-hydroxylase and aldosterone synthetase genes located on chromosome 8. As a result of this breakdown, both genes become sensitive to ACTH and aldosterone synthesis is initiated not only in the glomerular zone, but also in the fascicular zone of the adrenal cortex, which is accompanied by an increase in the production of aldosterone and metabolites of 11-deoxycortisol (18-oxocortisol and 18-hydroxycortisol).
The pathogenesis of primary hyperaldosteronism is associated with an excessive accumulation of sodium in the blood serum and an increase in the excretion of potassium in the urine. As a result, intracellular hypokalemia and partial replacement of potassium ions in the cell with hydrogen ions from the extracellular fluid are noted, which is accompanied by stimulation of chlorine excretion in the urine and causes the development of hypochloremic alkalosis. Persistent hypokalemia leads to damage to the renal tubules, which lose the ability to concentrate urine, and this is clinically accompanied by hypostenuria and secondary polydipsia. At the same time, hypokalemia leads to a decrease in sensitivity to ADH (antidiuretic hormone - vasopressin), which aggravates polyuria and polydipsia.
At the same time, hypernatremia causes water retention with the development of hypervolemia and arterial hypertension. It is fundamental that, in spite of sodium and fluid retention, edema (escape phenomenon) does not develop in primary hyperaldosteronism, which is explained by an increase in cardiac output, arterial hypertension and hypertensive diuresis.
Long-term presence of hyperaldosteronism is accompanied by complications caused by arterial hypertension (myocardial infarction, stroke) and specific myocardial hypertrophy. As mentioned above, persistent hypersecretion of aldosterone leads to progressive hypokalemia, which determines the development of hypokalemic myopathy, which leads to the appearance degenerative changes in the muscles.
Symptoms
Most patients have arterial diastolic hypertension, accompanied by headaches (arterial hypertension syndrome) and not amenable to treatment with antihypertensive drugs in medium therapeutic doses, hypertensive crises can be provoked by thiazide or loop diuretics and be accompanied by cardiac or cerebral symptoms.
An increase in blood pressure in combination with hypokalemia causes electrocardiographic disorders: there is a flattening or inversion of the T wave, a decrease segment S-T, lengthens q-T interval, a pronounced wave (wave) U appears. Cardiac arrhythmias and extrasystoles and signs of left ventricular hypertrophy are recorded. With primary hyperaldosteronism, edema is absent, while with secondary edema syndrome is the pathogenetic basis of the disease.
Hypokalemia, a characteristic symptom of hyperaldosteronism, predetermines the development of muscle weakness (myopathic syndrome), fatigue and decreased performance. Muscle weakness increases dramatically with exercise or suddenly (for no reason). In this case, the severity of weakness at the time of an attack limits the ability to move or minimal physical work. Paresthesias, local convulsions are possible.
As a result of impaired kidney ability to concentrate urine, polyuria with hypostenuria develops, often accompanied by secondary polydipsia. Characteristic symptom - with a predominance of nocturnal diuresis over daytime.
Depending on the degree of manifestation of the symptoms listed above, various options for the course of the disease are possible before the diagnosis is made:
- crisis option - accompanied hypertensive crises with severe neuromuscular symptoms (weakness, paresthesia, convulsions);
- a permanent form of arterial hypertension with constant muscle weakness, the degree of which is inferior to the crisis form;
- a variant without significant arterial hypertension with a predominance of transient neuromuscular disorders at the time of the crisis.
Diagnostics
Diagnosis of primary hyperaldosteronism includes two mandatory stages: proof of hyperaldosteronism and diagnosis of the nosological form of the disease.
The following indicators serve as evidence of primary hyperaldosteronism:
- serum potassium level
- the level of renin is reduced (plasma renin activity);
- the level of aldosterone in the blood is increased;
- the daily excretion of aldosterone metabolites in the urine (aldosterone-18-glucoronite) is increased.
The listed studies can be used in the examination of patients with arterial hypotension as screening methods for identifying the target group and conducting special examination... In difficult cases, pharmacodynamic tests can be used:
- test with isotonic sodium chloride solution: the patient is injected in a horizontal position with 2 liters of 0.9% sodium chloride solution slowly (for at least 4 hours) and after the end of the test the level of aldosterone is determined, which does not decrease with primary hyperaldosteronism;
- test with spironolactone: within 3 days the patient receives 400 mg / day of spironolactone orally. An increase in potassium levels of more than 1 mmol / l confirms hyperaldosteronism;
- test with furosemide: the patient is prescribed orally 0.08 g of furosemide. After 3 hours, there is a decrease in plasma renin activity and an increase in aldosterone levels in hyperaldosteronism;
- test with 9α-fluorocortisol: for 3 days the patient receives 400 μg / day orally of 9α-fluorocortisol (cortinefa) and the level of aldosterone is examined before and after the test With bilateral hyperplasia of the glomerular layer of the adrenal cortex, a decrease in the level of aldosterone is noted, and with aldosteroma, there is no decrease in the level of aldosterone:
- test with dexamethasone: used to differentiate glucocorticoid-suppressed hyperaldosteronism, the appointment of 0.5 - 1.0 mg 2 r / day for a week leads to a decrease in the manifestations of the disease;
- orthostatic test (allows to differentiate primary hyperaldosteronism with unilateral aldosteroma and bilateral adrenal hyperplasia): after 3-4 hours of the patient's stay in an upright position (standing, walking), the level of aldosterone and plasma renin activity are assessed. With autonomous aldosteroma, the plasma renin activity does not change (it remains low), and the aldosterone level decreases or changes slightly (normally, the plasma renin and aldosterone activity increase by 30% above the basal values).
Indirect signs of hyperaldosteronism:
- hypernatremia;
- hyperkaliuria, hypokalemia;
- polyuria, iso- and hypostenuria;
- metabolic alkalosis and increased serum bicarbonate levels (the result of the loss of hydrogen ions in the urine and impaired reabsorption of bicarbonate), as well as an alkaline urine reaction;
- in severe hypokalemia, the level of magnesium in the blood serum also decreases.
Criteria for the diagnosis of primary hyperaldosteronism include:
- diastolic hypertension in the absence of edema;
- decreased renin secretion (low plasma renin activity) without a tendency to an adequate increase in conditions of volume reduction (orthostasis, sodium restriction);
- hypersecretion of aldosterone, which is not sufficiently reduced under conditions of increasing volume (salt load).
As mentioned above, the cause of primary hyperaldosteronism can be established with some functional tests (orthostatic test, test with 9α-fluorocortisol). In addition, in familial hyperaldosteronism, suppressed by glucocorticoids and with preserved sensitivity to pituitary ACTH (familial type I hyperaldosteronism) and bilateral adrenal hyperplasia, there is an increase in the precursor levels in the synthesis of aldosterone - 18-hydroxycorticosterone - 18-hydroxycorticosterone /\u003e urine 18-hydroxycortisol\u003e 60 mg / day and 18-hydroxycortisol\u003e 15 mg / day. These changes are most pronounced in familial hyperaldosteronism, suppressed by glucocorticosteroids.
After verification of hyperaldosteronism, an additional examination is carried out aimed at clarifying the nosological form of primary hyperaldosteronism and topical diagnosis. First of all, the adrenal glands are visualized. The preferred methods are CG, MRI and PET. Revealed bilateral symmetric pathology or unilateral space-occupying mass in the adrenal gland makes it possible to establish the cause of primary hyperaldosteronism. It should be remembered that visualization of the adrenal glands is important only in view of the identified metabolic disorders.
In recent years, the list of possible evidence for primary hyperaldosteronism has been supplemented by the possibility of isolated blood sampling from the inferior vena cava and adrenal veins with a study of aldosterone levels in samples. An increase in the level of aldosterone by 3 times is considered characteristic of aldosteroma, less than 3 times - it is a sign of bilateral hyperplasia of the glomerular adrenal cortex.
Differential diagnosis is carried out with all conditions accompanying hyperaldosteronism. The principles of differential diagnosis are based on examination and exclusion different forms hyperaldosteronism.
Syndromes mimicking primary hyperaldosteronism include a number of diseases characterized by arterial hypertension and myopathic syndrome due to hypochloremic alkalosis and low renin levels (pseudohyperaldosteronism), are rare and are caused by various fermentopathies. At the same time, there is a deficiency of enzymes involved in the synthesis of glucocorticosteroids (11-β-hydroxylase, 11-β-hydroxysteroid dehydrogenase, 5α-reductase, P450c11, P450c17).
In most cases, syndromes mimicking primary hyperaldosteronism are manifested in childhood and are characterized by persistent arterial hypertension, as well as other laboratory signs hyperaldosteronism.
Treatment
Treatment of primary hyperaldosteronism is carried out taking into account the cause that caused it.
When aldosteroma is detected, the only treatment is surgery (adrenalectomy). Preoperative preparation is carried out for 4 - 8 weeks with spironolactone at a dose of 200 - 400 mg / day. With unilateral adrenalectomy, glucocorticosteroid replacement therapy is not indicated in the vast majority of cases. After removal of the adenoma, the cure of hypertension is observed in 55-60% of patients. However, arterial hypertension may persist in about 30% of operated patients.
If bilateral adrenal hyperplasia is suspected, surgical intervention is indicated only in cases where severe and accompanied clinical symptoms hypokalemia cannot be stopped with medication with spironolactone. Bilateral adrenalectomy, as a rule, does not improve the course of hypertension associated with idiopathic hyperplasia of the glomerular zone of the adrenal glands, therefore, in such cases, complex antihypertensive therapy is recommended with the obligatory use of maximum doses of spironolactone.
With familial glucocorticoid-suppressed hyperaldosteronism, suppressive therapy with dexamethasone at a dose of 0.5-1.0 mg / day is used.
RCHD (Republican Center for Healthcare Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical protocols MH RK - 2017
Primary hyperaldosteronism (E26.0)
Endocrinology
general information
Short description
Approved
Joint Commission on the Quality of Medical Services
Ministry of Health of the Republic of Kazakhstan
dated August 18, 2017
Protocol No. 26
PGA- a collective diagnosis characterized by an increased level of aldosterone, which is relatively autonomous from the renin-angiotensin system and does not decrease with sodium loading. Increased aldosterone levels cause cardiovascular disorders, decreased plasma renin levels, arterial hypertension, sodium retention, and increased potassium excretion, resulting in hypokalemia. Among the causes of PHA are adrenal adenoma, unilateral or bilateral suprarenal hyperplasia, in rare cases - hereditary HZHA.
INTRODUCTORY PART
ICD code (s):
Date of development / revision of the protocol:2013 (revised 2017).
Abbreviations used in the protocol:
| AG | - | arterial hypertension |
| HELL | - | blood pressure |
| APA | - | aldosterone-producing adenoma |
| APRA | - | aldosterone-producing renin-sensitive adenoma |
| APF | - | angiotensin converting enzyme |
| ARS | - | aldosterone-renin ratio |
| GZGA | - | glucocorticoid-dependent hyperaldosteronism HPHA - glucocorticoid-suppressed hyperaldosteronism |
| IGA | - | idiopathic hyperaldosteronism |
| PGA | - | primary hyperaldosteronism |
| PGN | - | primary adrenal hyperplasia |
| RCC | - | direct concentration of renin |
| Ultrasound | - | ultrasonography |
Protocol users: general practitioners, endocrinologists, internists, cardiologists, surgeons and vascular surgeons.
Evidence level scale:
| AND | High quality meta-analysis, systematic review of RCTs, or large RCTs with very low likelihood (++) of bias whose results can be generalized to the relevant population |
| IN | High-quality (++) systematic review of cohort or case-control studies or high-quality (++) cohort or case-control studies with very low risk of bias or RCTs with low (+) risk of bias that can be generalized to the relevant population |
| FROM | A cohort or case-control study or controlled trial without randomization with a low risk of bias (+), the results of which can be generalized to the relevant population, or RCTs with a very low or low risk of bias (++ or +), the results of which cannot be directly extended to the relevant population |
| D | Case series description or uncontrolled research or expert opinion |
| GPP | Best Clinical Practice |
Classification
Etiopathogenetic and clinical and morphological signs of PHA (E. G. Biglieri, J. D. Baxter, modification).
· Aldosterone-producing adenoma of the adrenal cortex (APA) - aldosteroma (Conn's syndrome);
Bilateral hyperplasia or adenomatosis of the adrenal cortex:
- idiopathic hyperaldosteronism (IHA, unsuppressed hyperproduction of aldosterone);
- undefined hyperaldosteronism (selectively suppressed production of aldosterone);
- glucocorticoid-suppressed hyperaldosteronism (HPHA);
· Aldosterone-producing, glucocorticoid-suppressed adenoma;
· Carcinoma of the adrenal cortex;
· Extra-adrenal hyperaldosteronism (ovaries, intestines, thyroid gland).
Diagnostics
DIAGNOSTIC METHODS, APPROACHES AND PROCEDURES
Diagnostic criteria
Complaints and anamnesis
: headaches, increased blood pressure, muscle weakness, especially in the calf muscles, cramps, parasthesia in the legs, polyuria, nocturia, polydipsia. The onset of the disease is gradual, symptoms appear after 40 years, more often diagnosed in 3-4 decades of life.
Physical examination:
· Hypertensive, neurological and urinary syndromes.
Laboratory research:
· Determination of potassium in blood serum;
· Determination of the level of aldosterone in blood plasma;
· Determination of the aldosterone-renin ratio (ARS).
Patients with a positive APC are recommended to undergo one of 4 confirmatory PHA tests prior to differential diagnosis of PHA forms (A).
Tests confirming PHA
|
Confirming PHA test |
Methodology | Interpretation | Comments |
|
Sodium test load |
Increase sodium intake\u003e 200 mmol (~ 6 g) per day for 3 days, under the control of daily sodium excretion, constant control of normokalemia while taking potassium preparations. The daily excretion of aldosterone is determined from the morning of the 3rd day of the test. | PHA is unlikely if the daily excretion of aldosterone is less than 10 mg or 27.7 nmol (excluding cases of chronic renal failure, in which the excretion of aldosterone is reduced). The diagnosis of PHA is highly probable with a daily excretion of aldosterone\u003e 12 mg (\u003e 33.3 nmod) according to the Mayo Clinic, and\u003e 14 mg (38.8 nmol) according to the Cleveland Clinic. | The test is contraindicated in severe forms of hypertension, chronic renal failure, heart failure, arrhythmias, or severe hypokalemia. Collection of daily urine is inconvenient. The diagnostic accuracy is reduced due to laboratory problems with the radioimmunoassay method (18-oxo - aldosterone glucuronide, a metabolite unstable in an acidic environment). Currently available and most preferred HPLC tandem mass spectrometry... With CRF, there may be no increased release of 18-oxoglucoronide aldosterone |
| Saline test | Lying position 1 hour before the start of the morning (8:00 - 9:30) 4-hour intravenous infusion of 2 liters of 0.9% NaCl. Blood on rhenium, aldosterone, cortisone, potassium at the basal point and after 4 hours. Monitoring blood pressure, heart rate during the test. | PHA is unlikely with post-infusion aldosterone levels of 10 ng / dL. Gray zone between 5 and 10 ng / dL | The test is contraindicated in severe forms of hypertension, chronic renal failure, heart failure, arrhythmias or severe hypokalemia. |
| Captopril test |
Patients receive 25-50 mg of captopril orally no earlier than one hour after the morning lifting. Blood sampling for ARP, aldosterone and cortisol is carried out before taking the drug and after 1-2 hours (all this while the patient is sitting) |
Normally, captopril reduces aldosterone levels by more than 30% from baseline. In PHA, aldosterone remains elevated with low ARP. With IHA, in contrast to APA, a slight decrease in aldosterone may be noted. | There are reports of a significant number of false negative and questionable results. |
Instrumental research:
· Ultrasound of the adrenal glands (however, the sensitivity of this method is insufficient, especially in the case of small lesions less than 1.0 cm in diameter)
· CT of the adrenal glands (the accuracy of detecting tumor formations with this method reaches 95%). Allows you to determine the size of the tumor, shape, topical location, to evaluate the accumulation and washout of contrast (confirms or excludes adrenocortical cancer). Criteria: benign lesions are usually homogeneous, their density is low, the contours are clear;
· Scintigraphy with 131 I-cholesterol - criteria: aldosteroma is characterized by asymmetric accumulation of the radiopharmaceutical (in one adrenal gland), in contrast to bilateral diffuse small-nodular hyperplasia of the adrenal cortex;
· Selective catheterization of the adrenal veins and determination of the level of aldosterone and cortisol in the blood flowing from the right and left adrenal glands (blood samples are taken from both veins of the adrenal glands, as well as from the inferior vena cava). Criteria: A fivefold increase in the aldosterone / cortisol ratio is considered confirmation of the presence of an aldosteroma.
Indications for specialist consultation:
· Consultation with a cardiologist in order to select antihypertensive therapy;
· Consultation of an endocrinologist in order to choose a treatment strategy;
· Consultation of a vascular surgeon for choosing a method of surgical treatment.
Diagnostic algorithm:(diagram)

APC is currently the most reliable and affordable method for PHA screening. When determining APC, as with other biochemical tests, false positive and false negative results are possible. APC is regarded as a test used for primary diagnosis, with dubious results due to various external influences (medication, non-compliance with the conditions for blood sampling). The effect of drugs and laboratory conditions on ARS is shown in Table 2.
Table 2. Drugs with a minimal effect on the level of aldosterone, with which we can control blood pressure in the diagnosis of PHA
| Drug group | International non-proprietary drug name | Mode of application | Comment |
|
nondihydropyridine calcium blocker channels |
Verapamil, prolonged form | 90-120 mg. twice a day |
Used alone or with others medicines from this table |
| vasodilator | * Hydralazine |
10-12.5 mg. twice a day with dose titration to effect |
It is prescribed after verapamil, as stabilizer of reflex tachycardia. Low dose administration reduces risk side effects (headache, tremor) |
|
Blocker a-adrenergic receptors |
* Prazosin hydrochloride |
0.5-1 mg two - three once a day with dose titration before effect |
Control of postural hypotension! |
Measurement of the aldosterone-renin ratio:
A. Preparing to identify ADR
1. Correction of hypokalemia after plasma potassium measurement is required. To exclude artifacts and overestimate the real level of potassium, blood sampling must meet the following conditions:
· Carried out by the syringe method (it is undesirable with a vacutainer);
· Avoid clenching the fist;
· Collect blood no earlier than 5 seconds after removing the turnstile;
· Separation of plasma at least 30 minutes after sampling.
2. The patient should not limit sodium intake.
3. To cancel drugs that affect the APC values \u200b\u200bat least 4 weeks before:
Spironolactone, triamterene;
Diuretics;
· Products from licorice root.
4. If the results of ARS against the background of taking the aforementioned drugs are not diagnostic, and if hypertension is controlled by drugs with a minimal effect on the level of aldosterone (see table 2) - cancel for at least 2 weeks other drugs that may affect the level of ARS :
Beta-blockers, central alpha-adrenergic agonists (clonidine, a-methyldopa), NSAIDs;
ACE inhibitors, angiotensin receptor blockers, renin inhibitors, dihydropyridine calcium channel blockers.
5. If it is necessary to control hypertension, treatment is carried out with drugs with minimal effect on the level of aldosterone (see table 2).
6. It is necessary to have information about the use of oral contraceptives (OC) and hormone replacement therapy, because estrogen-containing drugs can lower the direct renin concentration, which will cause a false-positive APC result. Do not cancel OK, in this case use the ATM level, not the RPC.
B. Sampling conditions:
· A fence in the morning, after the patient has been in an upright position for 2 hours, after being in a sitting position for about 5-15 minutes.
· Sampling in accordance with A. 1, stasis and hemolysis require re-sampling.
· Before centrifugation, keep the test tube at room temperature (and not on ice, since the cold regime increases APP); after centrifugation, the plasma component should be rapidly frozen.
C. Factors influencing the interpretation of results:
· Age\u003e 65 years affects a decrease in the level of renin, ARS is artificially increased;
· Time of day, food (salt) diet, time period of postural position;
· Medicines;
· Violations of the method of blood sampling;
Potassium level;
· Creatinine level (renal failure leads to false positive ARS).
Differential diagnosis
Differential diagnosis and justification of additional research
Table 3. Diagnostic tests for PHA
| Diagnostic test | Adrenal adenoma | Adrenal hyperplasia | ||
| APA | APRA | IGA | PGN | |
| Orthostatic test (determination in plasma of aldosterone after being in an upright position for 2 hours |
Decrease or no change |
Magnification |
Magnification |
Decrease or no change |
|
18-hydrocorticosterone serum |
\u003e 100 ng / dL |
\u003e 100 ng / dL |
< 100 нг/дл |
\u003e 100 ng / dL |
|
Excretion of 18-hydroxycortisol |
\u003e 60 μg / day |
< 60 мкг/сут |
< 60 мкг/сут |
\u003e 60 μg / day |
| Excretion of tetra-hydro-18-hydroxy-cortisol |
\u003e 15 mcg / day |
< 15 мкг/сут |
< 15 мкг/сут | < 15 мкг/сут |
|
Computed tomography of the adrenal glands |
Knot on one side | Knot on one side |
Bilateral hyperplasia, ± nodes |
Unilateral hyperplasia, ± knots |
|
Adrenal vein catheterization |
Lateralization | Lateralization | No lateralization | No lateralization |
Treatment
Preparations ( active ingredients) used in the treatment
Groups of drugs according to ATC used in treatment
Treatment (outpatient clinic)
TREATMENT TACTICS AT THE AMBULATORY LEVEL: only in the case of preoperative preparation (see the step-by-step patient management chart):
1) the appointment of an aldosterone antagonist - spironolactone at an initial dose of 50 mg 2 times a day with a further increase in 7 days to an average dose of 200 - 400 mg / day in 3 - 4 doses. If ineffective, the dose is increased to 600 mg / day;
2) in order to lower blood pressure until the potassium level normalizes, dihydropyridine calcium channel blockers at a dose of 30-90 mg / day can be prescribed;
3) correction of hypokalemia (potassium-sparing diuretics, potassium preparations);
4) Spironolactone is used for the treatment of IHA. In cases of erectile dysfunction in men, it can be replaced with amiloride * at a dose of 10-30 mg / day in 2 divided doses or triamterene up to 300 mg / day in 2-4 doses. These drugs normalize potassium levels, but do not lower blood pressure, and therefore it is necessary to add saluretics, calcium antagonists, ACE inhibitors and angiotensin II antagonists;
5) in the case of HPHA, dexamethasone is prescribed in individually selected doses necessary to eliminate hypokalemia, possibly in combination with antihypertensive drugs.
* apply after registration on the territory of the Republic of Kazakhstan
Non-drug treatment:
· Mode: sparing mode;
< 2 г/сут.
Drug treatment (preoperative preparation)
Essential Medicines List (having a 100% chance of being applied):
| Drug group | International non-proprietary drug name | Indications | Evidence level |
| Aldosterone antagonists | spironolactone | preoperative preparation | AND |
| Calcium antagonists | nifedipine, amlodipine | reduction and correction of blood pressure | AND |
| Sodium channel blockers |
triamterene amiloride |
potassium level correction | FROM |
List of additional medicines (less than 100% likely to be used): none.
Further management:
· Referral to a hospital for surgical treatment.
Surgical intervention: no.
· Stabilization of blood pressure;
· Normalization of potassium levels.
Treatment (hospital)
TACTICSSTATIONARY TREATMENT
Surgery (patient routing) 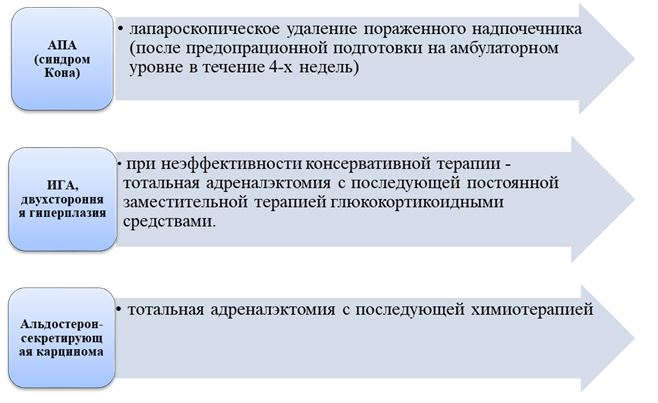
Non-drug treatment:
· Mode: sparing mode;
Diet: limiting table salt to< 2 г/сут.
Drug treatment:
List of essential drugs (100% likely to be used):
List of additional medicines (less than 100% likely to be used):
Further management: control of blood pressure to exclude relapses of the disease, lifelong intake of antihypertensive drugs in patients with IHA and HPHA, observation by a therapist and cardiologist.
Treatment effectiveness indicators:
· Controlled blood pressure, normalization of potassium levels in the blood.
Hospitalization
INDICATIONS FOR HOSPITALIZATION WITH INDICATION OF THE TYPE OF HOSPITALITY
Indications for planned hospitalization:
· For surgical treatment.
Indications for emergency hospitalization:
· Hypertensive crisis / stroke;
· Severe hypokalemia.
Information
Sources and Literature
- Minutes of meetings of the Joint Commission on the Quality of Medical Services of the Ministry of Health of the Republic of Kazakhstan, 2017
- 1) Primary hyperaldosteronism. clinical guidelines. Endocrine Surgery No. 2 (3), 2008, pp. 6-13. 2) Clinical endocrinology. Manual / Ed. N. T. Starkova. - 3rd ed., Rev. and add. - SPb .: Peter, 2002 .-- S. 354-364. - 576 p. 3) Endocrinology. Volume 1. Diseases of the pituitary gland, thyroid gland and adrenal glands. St. Petersburg. SpetsLit., 2011.4) Endocrinology. Edited by N. Lavin. Moscow. 1999. pp. 191-204. 5) Functional and topical diagnostics in endocrinology. S. B. Shustov., Yu.Sh. Halimov., G.E. Trufanov. P. 211-216. 6) Internal diseases. R. Harrison. Volume number 6. Moscow. 2005. p. 519-536. 7) Endocrinology according to Williams. Diseases of the adrenal cortex and endocrine arterial hypertension. Henry M. Cronenberg, Shlomo Melmed, Kenneth S. Polonsky, P. Reed Larsen. Moscow. 2010. p. 176-194. eight) Clinical guidelines "Incidentaloma of the adrenal glands (diagnosis and differential diagnosis)". Guidelines for doctors primary care... Moscow, 2015.9) Case Detection, Diagnosis, and Treatment of Patients with Primary Aldosteronism: An Endocrine Society Clinical Practice Guideline 10) John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata , Michael Stowasser, William F. Young, Jr; The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2016; 101 (5): 1889-1916. doi: 10.1210 / jc.2015-4061 11) Parthasarathy HK, Menard J, White WB, Young WF, Williams GH, Williams B, Ruilope LM, McInnes GT, Connell JM and MacDonald TM. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. Journal of hypertension, 2011, 29 (5), 980 12) Mulatero P, Rabbia F, Milan A, Paglieri C, Morello F, Chiandussi L, Veglio F. Drug effects on aldosterone / plasma renin activity ratio in primary aldosteronism. Hypertension. 2002 Dec; 40 (6): 897-902. 13) Pechère-Bertschi A, Herpin D, Lefebvre H. SFE / SFHTA / AFCE consensus on primary aldosteronism, part 7: Medical treatment of primary aldosteronism. Ann Endocrinol (Paris). 2016 Jul; 77 (3): 226-34. doi: 10.1016 / j.ando.2016.01.010. Epub 2016 Jun 14.
Information
ORGANIZATIONAL ASPECTS OF THE PROTOCOL
List of protocol developers:
1) Danyarova Laura Bakhytzhanovna - Candidate of Medical Sciences, endocrinologist, head of the endocrinology department of the Republican State Enterprise at the REM "Scientific Research Institute of Cardiology and Internal Diseases".
2) Raisova Aigul Muratovna - Candidate of Medical Sciences, Head of the Therapeutic Department of the Republican State Enterprise at the REM "Scientific Research Institute of Cardiology and Internal Diseases".
3) Smagulova Gaziza Azhmagievna - Candidate of Medical Sciences, Head of the Department of Propedeutics of Internal Diseases and Clinical Pharmacology of the Republican State Enterprise at the REM "West Kazakhstan State Medical University named after M. Ospanov".
No Conflict of Interest Statement:no.
Reviewers:
Bazarbekova Rimma Bazarbekovna - Doctor of Medical Sciences, Professor, Head of the Department of Endocrinology of JSC Kazakh Medical University of Continuing Education.
Indication of the conditions for revising the protocol:revision of the protocol 5 years after its publication and from the date of its entry into force or in the presence of new methods with a level of evidence.
Attached files
Attention!
- Self-medication can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" cannot and should not replace an in-person consultation with a doctor. Be sure to contact medical institutions if you have any medical conditions or symptoms that bother you.
- The choice of medicines and their dosage should be discussed with a specialist. Only a doctor can prescribe the right medicine and its dosage, taking into account the disease and the condition of the patient's body.
- MedElement website and mobile applications "MedElement (MedElement)", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" are exclusively informational and reference resources. The information posted on this site should not be used to unauthorized changes in the doctor's prescription.
- The MedElement editors are not responsible for any damage to health or material damage resulting from the use of this site.
The adrenal cortex is responsible for the synthesis of three groups of hormones. Including the cells of this endocrine organ produce mineralocorticoids. The main representative of this class of hormones is aldosterone.
Normally, aldosterone is secreted under the control of the renin-angiotensin blood system. The hormone increases urinary potassium loss and sodium retention.
If there is too much aldosterone, hyperaldosteronism is diagnosed. This condition can be caused by both adrenal pathology and systemic disorders.
Primary hyperaldosteronism is called Connes syndrome. This disease is based on excessive secretion of the hormone in the glomerular zone of the adrenal cortex.
Connes syndrome is three times more likely to be diagnosed in women than in men. Symptoms usually appear between the ages of 30 and 40.
Causes of primary hyperaldosteronism
Conn's syndrome can develop due to various pathological processes.
An excess of mineralocorticoid secretion is caused by:
- hyperplasia of the adrenal cortex;
- aldosteroma ( benign tumor glomerular zone);
- carcinoma (malignant tumor).
About 30-40% of primary hyperaldosteronism is associated with cortical hyperplasia. Unilateral adenoma is the cause of 60% of all cases of Connes syndrome. The frequency of malignant tumors is 0.7–1% in the morbidity structure.
The symptoms of hyperaldosteronism are the same for all etiological factors. Excessive secretion of the hormone in Conn's syndrome leads to severe electrolyte disturbances. Both tumors and the hyperplastic cortex do not respond to the regulatory action of the renin-angiotensin system. Primary hyperaldosteronism has the properties of autonomy, that is, independence.
The clinical picture of the syndrome
Primary hyperaldosteronism has three characteristic groups of symptoms.
Allocate:
- cardiovascular;
- neuromuscular;
- renal components.
Changes in the volume of circulating blood and disturbances in the work of the heart muscle are manifested by arterial hypertension, heart failure, vascular accidents (strokes, heart attacks).
Patients are worried about headaches, shortness of breath, decreased tolerance to physical activity, weakness, fatigue, heaviness behind the breastbone.
When blood pressure is monitored, persistent hypertension is recorded. Patients have high numbers of both systolic and diastolic pressure. Treatment of hypertension in Connes syndrome is practically ineffectual. All modern antihypertensive drugs and their combinations cannot maintain normal blood pressure in the patient.
As a result, target organ damage develops rapidly. On the fundus, on examination, angiopathy, hemorrhages, and retinal detachment can be detected. In severe cases, these changes cause blindness. The heart muscle undergoes hypertrophy. Thickening of the myocardial wall is accompanied by a violation of its oxygen supply and nutrients... Because of this, the heart becomes less resistant to stress. The left ventricular ejection fraction falls, heart failure appears.
The neuromuscular component of Connes syndrome is associated with a change in the ratio of potassium and sodium levels in the blood. Patients with primary hyperaldosteronism complain of muscle weakness, discomfort in the extremities (cold, "chills"), convulsions. Sometimes complete or partial paralysis can develop.
Kidney damage in primary hypercortisolism syndrome is explained by an excess of potassium in the urine. Patients are worried about strong thirst, dry mouth. The volume of urine per day may be higher than normal. Usually nocturnal urine output prevails over daytime.
In urine tests, low density, alkaline reaction, proteinuria (protein) are detected. Long-term primary hyperaldosteronism can cause chronic renal failure.
Examination for hyperaldosteronism syndrome
If the doctor suspects the patient's Connes syndrome, then further it is necessary to undergo a diagnostic examination.
To clarify the condition, you need:
- identify high levels of aldosterone;
- prove the primary nature of the disease;
- assess the condition of the adrenal glands (find a tumor).
It is not always easy to assess the concentration of a hormone in the blood. Aldosterone levels, even in Connes syndrome, are prone to rapid changes. The most accurate study is the analysis for the ratio of aldosterone and plasma renin. In addition, the patient must determine the level of potassium in the blood.
In primary hyperaldosteronism, aldosterone is above normal, potassium and renin are reduced.
Special tests have been proposed and successfully used for diagnostics. They are usually carried out in a hospital after hospitalization.
Endocrinologists conduct tests:
- with sodium chloride;
- with hypothiazide;
- with spironolactone.
Assessment of the state of the adrenal cortex is possible in different ways. Diagnostics start with ultrasound examination... Further more accurate computed tomography may be required.
If the tumor is small (up to 1 cm), then angiography is considered the most informative. it is desirable to combine it with blood samples from the vessels of the adrenal glands.
Treatment of the disease
Primary hyperaldosteronism begins to be treated conservatively. The patient is prescribed spironolactone tablets. In addition, antihypertensive and cardiovascular drugs are used. Further tactics depend on the results of ultrasound and tomography. If a tumor is found in the adrenal glands, then a surgical operation is required. After removal of the formation, it is examined under a microscope. If signs of malignancy are found, then the oncologist determines the further tactics.
In the event that there is no volumetric neoplasm in the adrenal glands, then surgery not necessary. The patient continues to receive drugs according to the scheme and regularly undergoes a control examination. Endocrinologist visits are required every few months. Monitoring of blood tests is needed even more often. Medical supervision includes assessment of symptoms, measurement of blood pressure, electrocardiogram, blood sampling for electrolytes, aldosterone, plasma renin. Every year, all patients with primary idiopathic hyperaldosteronism are recommended to undergo an ultrasound of the adrenal glands, computed tomography or angiography. If a tumor is found in one of the control examinations, then surgical treatment is recommended. The operation is performed after planned preparation (correction of blood composition and cardiac activity).