Proximal phalanx of the finger. Proximal phalanx Proximal phalanx 5th toe
Fractures of the middle and proximal phalanges have much in common both in the mechanisms of damage and treatment, which allows them to be considered together, but taking into account differences.
TO proximal phalanx tendons are not attached. However, some tendons that run close to it can complicate the treatment of fractures. Fractures of the proximal phalanges have a tendency to angular deformity towards the palm due to the predominance of traction of the interosseous muscles over the extensor tendons.
Fractures of the middle phalanges are less common than proximal ones due to the fact that most of the damaging force acting along the axis of the finger is absorbed by the proximal phalanx. This leads to frequent fractures and dislocations of the proximal but not the middle phalanges. Most fractures of the middle phalanx occur in its weakest part - the diaphysis. It is important to note that the superficial flexor is attached to almost the entire volar surface of the phalanx, while the insertion of the extensor tendon is limited to the proximal dorsal surface.
Tendon superficial flexor bifurcated and attached to the lateral and medial edges of the bone.
Having a wide area attachments, the superficial flexor develops significant force leading to deformity when the middle phalanx is fractured. For example, a fracture of the base of the middle phalanx usually results in displacement of the distal fragment towards the palm, while a fracture of the diaphysis is usually accompanied by displacement of the fragments at an angle open to the dorsal side.
Last anatomical feature which should be taken into account is the presence of a cartilaginous plate on the palmar side of the base of the middle phalanx. Intra-articular fractures can be complicated by displacement of this cartilaginous plate.
Classification of fractures of the proximal and middle phalanges of the fingers
Fractures of the proximal and middle phalanges divided into three types. Type I fractures - stable, non-displaced, can be treated by a doctor emergency care. In type II fractures, displacement is possible, after reposition they can remain both stable and unstable. Patients with type II fractures should be referred for orthopedic treatment. Type III fractures are unstable and often complicated by rotational displacement. Reposition them surgically.
These patients require careful surveys with fixation of the nerve function distal to the fracture site. In the treatment of fractures of this type, it is necessary to identify and correct rotational displacement. Rotational deformity may be suspected when not all of the fingers of the clenched fist point to the scaphoid. Another diagnostic method is to compare the direction of the lines of the nail plates on each hand. Normally, the line of the nail plate of the extended third finger of the right hand will pass in the same plane as the line of the third finger of the left hand. With rotational displacement, these lines will not be parallel.
Rotational displacement can be identified by comparing the diameter of the bone fragments of the phalanx. It should be suspected in case of asymmetry of these fragments.
 With rotational displacement, the lines of the nail plates are not parallel compared to the nail plates of the fingers of an intact hand.
With rotational displacement, the lines of the nail plates are not parallel compared to the nail plates of the fingers of an intact hand.
Treatment of fractures of the middle and proximal phalanges of the fingers
In the treatment of fractures of the middle and proximal phalanges there are two main principles:
1. The finger should never be immobilized in full extension. The finger should be immobilized in a functionally advantageous position: 50° flexion at the metacarpophalangeal and 15-20° flexion at the interphalangeal joints to prevent stiffness and contractures. If stable fixation of fragments is possible only with full extension, then for immobilization in the flexion position, internal fixation is required. In the flexion position, the repositioning collateral ligaments are stretched.
2. Never apply a cast proximal to the distal palmar crease. If a wider immobilization is required, a grooved splint should be used that captures the adjacent healthy finger along with the injured finger, or a plaster cast with a traction device.
There are three methods of treatment fractures of the middle and proximal phalanges. The choice depends on the type of fracture, its stability, and the experience of the clinician.
Dynamic busting. This method of treatment consists in fixing the injured finger together with the adjacent healthy one. This allows maximum use of the hand with early onset of motion and prevents stiffness. The method is indicated only for stable fractures without displacement, as well as stable transverse or impacted fractures. It should not be used for fractures with angular or rotational displacement. The imposition of plaster bandages, splints and devices for traction.
These methods mainly used only by orthopedists or surgeons (with the exception of grooved splints). A grooved splint is used for stable fractures that do not need traction and are not complicated by rotational or angular displacement. The grooved splint provides more reliable immobilization than dynamic splinting. Traction devices are used for complicated fractures and are usually applied only after consulting an orthopedic surgeon.
Internal fixation. Typically, internal fixation with a Kirschner wire is performed for unstable or intra-articular avulsion fractures when precise reduction is required.
Since a person moves in a straight position, the lion's share of the load falls on the fate of the lower extremities. Therefore, it is important to monitor your body weight, making it easier for the bones of the foot to work.
The structure of the ankle joint in humans is represented as an articulation of the bones of the foot with the tibia between themselves, ensuring the performance of complex functions.
- Human ankle joint
- Circulatory and nervous systems of the foot
- Diagnostic measures
- Ankle and foot pathologies
Human ankle joint
The bones are clearly shown in the diagram and are classified into groups.
These include:
- The articulation of the leg bones with the bones of the foot.
- Internal articulation of the bones of the tarsus.
- Articulations between the bones of the metatarsus and tarsus.
- Articulations of the proximal phalanges with the bones of the metatarsus.
- The articulation of the phalanges of the fingers with each other.
The anatomical abilities of the foot suggest high level motor activity. For this reason, it is possible for a person to perform large physical exertion.
Both the foot and the whole leg are designed to help a person in free movement in the environment.
 The structure of the foot is divided into 3 working parts:
The structure of the foot is divided into 3 working parts:
- Bones.
- Ligaments.
- Muscles.
The skeletal base of the foot includes 3 sections: fingers, metatarsus and tarsus.
The design of the toes includes phalanges. Just like a brush thumb the foot consists of 2 phalanges, and the remaining 4 fingers - of 3.
Often there are cases when 2 components of the 5th finger grow together, forming a finger structure of 2 phalanges.
The structure has proximal, distal and middle phalanges. They differ from the phalanges of the hand in that their length is shorter. A clear expression of this is seen in the distal phalanges.
The bones of the tarsus of the posterior section are composed of the talus and calcaneal components, and the posterior section is subdivided into the cuboid, scaphoid and sphenoid bones.
The talus is located at a distance from the distal end of the tibia, becoming a bony meniscus between the bones of the foot and knee.
It consists of a head, neck, and body, and is designed to connect to the tibia, ankles, and calcaneus.
The calcaneus is part of the posterior lower lobe of the tarsus. It is the largest part of the foot and has an elongated, laterally flattened appearance. Along with this, the calcaneus is the link between the cuboid and the talus.
The navicular bone is located on the inside of the foot. It has a convex forward appearance with articular components connecting to closely spaced bones.
The cuboid part is located on the outer side of the foot, articulating with the calcaneus, scaphoid, sphenoid and metatarsal bones. Below the cuboid bone is a groove, into which the tendon of the elongated peroneal muscle is laid.
The composition of the sphenoid bones includes:
- medial.
- Intermediate.
- Lateral.
They lie in front of the scaphoid, inward from the cuboid, behind the first 3 metatarsal fragments and represent the anterior inner part of the tarsus.
The skeleton of the metatarsus is presented in segments of a tubular shape, consisting of a head, body and base, where the body is similar to a trihedral prism. In this case, the longest bone is the second, and the thickened and short one is the first.
The bases of the bones of the metatarsus are equipped with articular surfaces that serve as a connection with the bone components of the tarsus. In addition, it articulates with nearby bones of the metatarsus. At the same time, the heads provided with articular surfaces are connected to the proximal phalanges.
The metatarsals are easily palpated due to the relatively thin soft tissue coverage. They are placed in different-angled planes, creating a vault in the transverse line.
Circulatory and nervous systems of the foot
Nerve endings and blood arteries are considered an important component of the foot.
There are 2 main arteries of the foot:
- Rear.
- Posterior tibial.
 Also circulatory system includes small arteries distributing to all parts of the tissues.
Also circulatory system includes small arteries distributing to all parts of the tissues.
Due to the remoteness of the arteries of the feet from the heart, circulatory disorders are often recorded due to oxygen deficiency. The results of this are manifested in the form of atherosclerosis.
The longest vein that carries blood to the heart is located on a segment from the point of the thumb, extending inside the leg. It is commonly called the great saphenous vein. At the same time, the small saphenous vein passes along the outer side of the leg.
The tibial anterior and posterior veins are placed deep into the leg, and small ones drive blood into large veins. Moreover, small arteries supply tissues with blood, and the smallest capillaries join veins and arteries.
A person suffering from circulatory disorders notes the presence of edema in the afternoon. Moreover, it may appear varicose veins veins.
As in other parts of the body, in the foot, the nerve roots read all the sensations and transmit them to the brain, controlling movement.
TO nervous system feet are:
- Superficial peroneal.
- Deep peroneal.
- Posterior tibial.
- Calf.
Tight shoes can pinch a nerve, causing swelling, which will lead to discomfort, numbness and pain.
Diagnostic measures
At the moment when alarming symptoms occur in the foot area, a person comes to an orthopedist and traumatologist, who, knowing the full structure of the ankle joint, can determine a lot by external signs. But at the same time, specialists prescribe an examination necessary for a 100% correct diagnosis.
Survey methods include:
- X-ray examination.
- Ultrasonography.
- Computed and magnetic resonance imaging.
- Athroscopy.
 Detection of pathologies through x-rays is the most budgetary option. Pictures are taken from several sides, fixing the probable dislocation, swelling, fracture and other processes.
Detection of pathologies through x-rays is the most budgetary option. Pictures are taken from several sides, fixing the probable dislocation, swelling, fracture and other processes.
Ultrasound helps to detect the concentration of blood, finding foreign bodies, a possible edematous process in the articular bag, as well as check the condition of the ligaments.
Computed tomography provides a complete examination bone tissue, with neoplasms, fractures and arthrosis. Magnetic resonance imaging is an expensive research technique that brings maximum reliable information about the Achilles tendon, ligaments and articular cartilage.
Atroscopy is a small invasive intervention, which implies the insertion of a special camera into the joint capsule, due to which the doctor can see all the pathologies of the ankle joint.
After collecting all the information with instrumental and hardware tools, examining doctors and obtaining the results of laboratory tests, an accurate diagnosis is made with the definition of a treatment method.
Ankle and foot pathologies
Frequent pain, external changes, swelling and impaired motor functions can serve as signs of foot ailments.
As a rule, a person may experience the following diseases:
- Arthrosis in the ankle joint.
- Arthrosis of the toes.
- Valgus change of the thumb.
Arthrosis of the ankle joint is characterized by crunching, pain, swelling, fatigue during running and walking. This is due to the course of the inflammatory process that damages the cartilage tissue, leading to a typical deformation of the tissues of the joints.
The causes of the disease can be constant increased loads and injuries that provoke the development of dysplasia, osteodystrophy and negative changes in statics.
Treatment is carried out based on the degree of arthrosis with drugs that reduce pain, restore blood circulation and block the spread of the disease. In difficult cases, surgical intervention, relieving the patient of damaged segments of the joint, recreating mobility and eliminating pain.
Arthrosis of the toes is noted in the course of metabolic disturbances and typical blood circulation in the metatarsophalangeal joints. This is facilitated by the lack of moderation in loads, uncomfortable narrow shoes, injuries, excess weight and frequent hypothermia.
The symptoms of the disease include swelling, deformation of the structure of the fingers, pain during movement and a crunch.
 On the initial stage arthrosis of the fingers, measures are taken to avoid deformation, with pain relief. If an advanced stage is detected, in most cases, the doctor prescribes arthrodesis, arthroplasty or arthroplasty in an operative way, which should completely solve the problem of the disease.
On the initial stage arthrosis of the fingers, measures are taken to avoid deformation, with pain relief. If an advanced stage is detected, in most cases, the doctor prescribes arthrodesis, arthroplasty or arthroplasty in an operative way, which should completely solve the problem of the disease.
Hallux valgus, better known as a "bump" at the base of the thumb. This disease is characterized by the displacement of the head of one phalangeal bone, the declination of the thumb to the other four, the weakening of the muscles and the resulting deformity of the foot.
Treatment that inhibits the development of the disease is determined by prescribing baths, physiotherapy, and physiotherapy exercises. When the form of changes becomes pronounced, an operation is performed, the method of which is determined by the attending orthopedist, taking into account the stage of the disease and the general well-being of the patient.
Why do fingers hurt: causes of pain in the joints of the fingers of the right and left hands
To learn more…
Pain in the small joints of the fingers and toes is a fairly common phenomenon and at first glance seems safe.
Most often, this condition is observed in people after forty years, however, there are many diseases in which pain in the fingers of the right or left hand occurs in the younger generation.
The human musculoskeletal system includes more than 300 small and large joints. The most mobile are in the fingers and toes. These joints have a thin connective sheath and a small articular surface.
That is why they are so often damaged and diseased.
A joint is a connection of terminal bones covered with hyaline cartilage. The articulation site is covered with a synovial membrane, which contains articular exudate.
Each finger of the hand (middle, little finger, index, ring, except for the thumb) consists of three phalanges:
- Proximal.
- Average.
- Distal.
In addition, they have three joints:
- Proximal - connect the bones that form the palm with the proximal phalanx of the finger.
- Middle phalanx - connects the proximal and middle phalanx.
- Distal - with the help of it, the middle phalanx articulates with the distal.
Why does pain appear in the fingers? The reason for this condition is inflammatory diseases of the joints and traumatic injuries.
Diseases that damage the joint
Pain in the fingers and toes can occur due to the following diseases:
- Arthritis (psoriatic, stenosing, infectious, reactive, rheumatoid).
- Arthrosis.
- Gout.
- Bursitis.
- Osteoarthritis.
- Osteomyelitis.
- Tendovaginitis.
- De Quervain's disease.
- Raynaud's syndrome.
- Angiospastic peripheral crisis
That is why there may be pain in the fingers, both in the right and in the left limb. And now more about each disease.
Arthritis
Arthritis is a whole group of pathologies for which it is typical acute inflammation elements of the joint and adjacent tissues.
With any type of arthritis, pain sensations in the fingers and toes appear not only when the limb is performing any actions, but also in a state of complete rest.
Moreover, the pains are intense, in the morning stiffness is noted in the joints. During loads, crepitus (crunching), an increase in local temperature and deformation of the joint are possible.
Rheumatoid arthritis - pathology connective tissue combined type. For rheumatoid arthritis, damage to small joints is typical (little fingers and other fingers of the left or right hand).
Symptoms of rheumatoid arthritis:
- inflammation of the metacarpophalangeal joints of the fingers;
- symmetry - if inflammation develops on the right hand, it will certainly affect the other limb.
This disease is insidious in that when it appears, there is a high risk of involvement in the inflammatory process of large joints: knee, elbow, ankle, hip.
Pain rheumatoid arthritis usually occurs at night and in the morning.
Gout
Gout or gouty arthritis is another type of arthritis. The cause of the disease is an excessive accumulation of uric acid in the body, the crystals of which settle on soft and hard tissues and destroy the joint.
Previously, only rich people suffered from gout, who could afford excesses in food: fatty meat and fish, alcoholic beverages.
Meat is the main source of purines, which lead to the development of gouty arthritis. Gout usually affects the big toes.
Symptoms:
- pain in the big toes;
- if the disease covers the joints of the right or left hand, we can talk about the development of polyarthritis;
- the joint is red and swollen.
For a gouty attack:
- the joints of the toes are very swollen;
- the pain is burning, it mainly occurs at night;
- there is a local increase in temperature.
On average, a gout attack lasts from three days to several weeks. characteristic feature gouty arthritis is the formation of tophi - pathological compacted nodules that do not cause pain to the patient and are only a cosmetic defect.
Psoriatic arthritis is a form of psoriasis. In addition to being amazed skin, there is inflammation in the joints of the legs and arms (right or left). This type of arthritis affects all joints of one finger at once. The inflamed finger is red and swollen. The joints are affected asymmetrically.
Septic infectious arthritis occurs due to the penetration of infection into the tissue of the joint through damaged areas of the skin or through the blood. It can hurt only one joint or several at once. The intensity of the symptoms of the disease depends on the stage of its development.
For purulent or advanced inflammation, the following symptoms are characteristic:
- fever;
- severe intoxication;
- body temperature rises to a critical level.
V childhood the symptoms of the disease are more pronounced, which cannot be said about the pathology that develops in an adult.
Other joint diseases
Stenosing ligamentitis is characterized by inflammation of the annular ligament of the fingers of the right or left hand.
Symptoms of the disease
- numbness;
- severe burning;
- cyanosis and swelling of the finger;
- pain affects all fingers, but does not affect the little finger.
- the joint cannot be extended without the application of external forces.
Discomfort and pain intensify at night and in the morning. During the day, the pain disappears completely.
In osteoarthritis, cartilage is destroyed in the joint. Women during menopause are more susceptible to this disease.
Causes of osteoarthritis:
- hereditary factors;
- hormonal disorders;
- metabolic disease;
- occupational workloads.
Symptoms of osteoarthritis:
- stiffness of the right or left hand in the morning;
- limited mobility in the joints;
- crepitus when working with hands;
- with a load on the joint, pain appears, which subsides at night;
- dull pains at night are possible with venous congestion.
At first, the disease affects only one joint, after which the remaining joints are involved in the inflammatory process. Secondary lesions are those diarthrosis, which during the first inflammation took over all the work.
If only the joint of the thumb on the right hand hurts, the doctor may suspect rhizarthrosis, a type of osteoarthritis. For this disease, damage to the base of the joint, which connects the metacarpal and radiocarpal bones, is typical.
Rhizarthrosis can be triggered by constant stress on the muscles and joints of the thumb. Signs of pathology include pain and deformity of the bones of the thumb.
Osteomyelitis is a purulent-necrotic process that can occur in the bones of the arms and legs, bone marrow, soft tissues and joints. The causes of osteomyelitis are pus-producing bacteria.
The main symptoms of the onset of the disease:
- severe intoxication;
- a significant increase in temperature;
- nausea and vomiting;
- joint pain;
- chills;
- deterioration in general condition;
- headache.
If osteomyelitis has been going on for several days, additional symptoms appear:
- limitation of active and passive movement of the hands;
- swelling of the muscles of the hand;
- the appearance of a venous pattern on the skin is possible;
- intensification of pain.
Even if the pain in the joints, intoxication and temperature have eased somewhat, this is not at all evidence that the disease is receding. On the contrary, these signs may indicate the transition of the disease to the chronic stage.
Fistulas often appear on the affected areas, from which pus is released in small quantities. Drainage of fistulas forms subcutaneous channels, leads to curvature of the fingers and their immobility.
Bursitis is a disease in which joint bags become inflamed, and fluid accumulates in the joint cavity.
Bursitis symptoms:
- sharp pain on palpation;
- dark red skin tone;
- an increase in local temperature;
- the formation of a mobile and soft swelling.
If the cause of bursitis is an injury to the hand or finger, there is a possibility of developing a purulent form of bursitis, which is accompanied by:
- weakness in the whole body;
- pain in the limb;
- constant nausea;
- headache.
Angiospastic peripheral crisis is another reason pain in the fingers. The disease is accompanied by cold fingers, their cyanosis, and after a strong reddening of the skin. The cause of the pathology is hypothermia.
Injury or compression of the wrist joint may cause neuropathy of the ulnar nerve, in which the fingers hurt. The more neglected the disease, the more limited the functionality of the fingers at the time of abduction and adduction of the hand.
If the pain in the fingers is paroxysmal in nature and is accompanied by pallor of the tips, this pathology is called "Raynaud's syndrome". The disease can occur on its own or be a symptom of another disease.
The main signs of Raynaud's syndrome:
- white color of the fingertips;
- severe burning pain that occurs after stress or hypothermia.
The disease is dangerous because its presence in the body disrupts the process of delivering oxygen to cells and tissues, as a result of which the fingertips can become dead. All symptoms of the disease are directly related to the violation of peripheral blood circulation in the vessels.
De Quervain's disease is an inflammation of the thumb ligament. For pathology, the appearance of pain in the wrist joint is typical, which increases with the movements of the hand. Pain may radiate to the forearm, shoulder, and neck. On palpation in the affected area, swelling and severe pain are noted.
Tendovaginitis is a pathology characterized by acute or chronic inflammatory process in the connective tissue sheaths of the tendons.
Symptoms:
- pain during flexion and extension of the finger;
- crepitus with any movement;
- swelling in the area of the tendon sheath.
- Relieves pain and swelling in the joints with arthritis and arthrosis
- Restores joints and tissues, effective for osteochondrosis
To learn more…
| proximal phalanx(phalanx proximalis) Foot bones(ossa pcdis). View from above. 1-distal (nail) phalanges; |
|
 |
Foot bones(ossa pedis). Plantar side (view from below). A - bones of the tarsus, G - bones of the metatarsus, B - bones of the fingers 1-phalanx; |
- - closely closed linear formation of heavy infantry in Ancient Greece, Macedonia and Ancient Rome. Had 8-16 ranks. She had great striking power, but was inactive ...
Historical dictionary
- - the battle order of the Greek army in the form of a tightly closed formation of hoplites from 8-16, sometimes even 25 rows ...
Antique world. Dictionary-reference
- - closely close) th linear military formation, consisting of several. ranks of heavy infantry in Dr. Greece...
Dictionary of antiquity
- - order of battle in other Greek. troops in the form of a tightly closed linear formation of hoplites with a system depth of 8-16 rows. Along the front, F. occupied up to 500 m ...
Soviet historical encyclopedia
- - Phalanx, . The battle in the heroic era was, apparently, the battle of leaders alone ...
Real Dictionary of Classical Antiquities
- - see Kugelberg-Welander disease ...
Big Medical Dictionary
- - V. s., at which the branches intersect vagus nerve only to upper departments stomach...
Big Medical Dictionary
- - , closely closed linear construction of the Greek. infantry) for combat. F. had 8–16 rows, along the front it occupied up to 500 m ...
Great Soviet Encyclopedia
- - a lot - a hint at the phalanx among the ancients - an army, a detachment. Wed He is not alone here, but a whole phalanx of them ... Pisemsky. Forties people. 5, 12. Cf. a servant, powdered, in livery caftans ... gives her a place .....
Michelson Explanatory Phraseological Dictionary (original orph.)
- - ; pl. fala/ngi, R....
Spelling Dictionary of the Russian Language
- - Greek. row, system; | poisonous insect, centipede...
Dictionary Dalia
- - PHALANGE, -and, wives. 1. The ancient Greeks: close formation of infantry. 2. In the utopian socialism of C. Fourier: a large community, a commune. 3. In Spain: the name of the fascist party...
Explanatory dictionary of Ozhegov
- - PHALANGE, phalanges, female. . 1. The tightly closed formation of the infantry of the ancient Greeks. || trans. In general, a slender, closed row of someone or something. The phalanx of white pawns moved to attack the black king. 2...
Explanatory Dictionary of Ushakov
-
Explanatory Dictionary of Efremova
- - phalanx I 1. Each of the three short tubular bones that form the skeleton of the fingers of the limbs in humans and vertebrates. 2. see also. phalanx II. one...
Explanatory Dictionary of Efremova
- - phalanx I 1. Each of the three short tubular bones that form the skeleton of the fingers of the limbs in humans and vertebrates. 2. see also. phalanx II. one...
Explanatory Dictionary of Efremova
"Proximal phalanx" in books
PHALANX
From Fourier's book author Vasilkova Yulia ValerievnaPHALANX In contrast to the Theory of Four Movements, the Treatise is full of practical advice: how to create an association ... how best to arrange the life of the Harmonians ... Fourier groups humanity into phalanxes, borrowing this name from the ancient Greeks, from whom it meant
§ 5. Greek phalanx
From the book Antique City author Elizarov Evgeny Dmitrievich§ 5. The Greek phalanx Of course, one cannot see in all this the formation of a truly special breed of heroes who have become related to the immortal inhabitants of Olympus, victorious supermen, “blond beasts”, for whom there are no longer any barriers or
Macedonian phalanx
From the book Daily Life of the Army of Alexander the Great the author Fort PaulThe Macedonian phalanx From the infantry units of the Greeks, whether they were allies in the pan-Greek federation or mercenaries, the Macedonian phalanx (literally meaning “log”, “grinding roller”) differed not only and, perhaps, not so much in weapons or equipment, but before
Phalanx
From the book Greece and Rome [The evolution of military art over 12 centuries] author Connolly PeterPhalanx During the VIII century. BC. revolutionary changes took place in the military affairs of the ancient Greeks. Instead of the old principle of battle, when everyone fought the enemy "on his own", a system was now introduced that required much more discipline. Such a system was
"African Phalanx"
From the book Foreign Volunteers in the Wehrmacht. 1941-1945 author Yurado Carlos Caballero"African phalanx" After the landing of the allies in Northern France (Operation "Torch"), of all the North African territories of France, only Tunisia remained under the sovereignty of Vichy and the occupation of the "Axis" troops. After the landing, the Vichy regime made an attempt to create volunteer
Phalanx
From the book Greece and Rome, an encyclopedia of military history author Connolly PeterPhalanx During the VIII century. BC. revolutionary changes took place in the military affairs of the ancient Greeks. Instead of the old principle of battle, when everyone fought the enemy "on his own", a system was now introduced that required much more discipline. Such a system was
Chapter 2 Phalanx
From the book The Art of War: The Ancient World and the Middle Ages [SI] authorChapter 2 The Phalanx But the role of the infantry phalanx in Alexander's victories should not be underestimated either. Let's look at all the advantages and disadvantages of the Macedonian phalanx. I already said above in the section on the Greco-Persian wars that the main advantage of the phalanx is
Chapter 2 Phalanx
From the book The Art of War: The Ancient World and the Middle Ages author Andrienko Vladimir AlexandrovichChapter 2 The Phalanx But the role of the infantry phalanx in Alexander's victories should not be underestimated either. Let's look at all the advantages and disadvantages of the Macedonian phalanx. I already said above in the section on the Greco-Persian Wars that the main advantage of the phalanx is
Spanish phalanx
From the book Big Soviet Encyclopedia(IP) author TSBPhalanx
From the book Great Soviet Encyclopedia (FA) of the author TSBSalpuga or phalanx
From the book I know the world. Insects the author Lyakhov PetrSalpuga or phalanx Solpugi, or as they are also called phalanges, make up a separate detachment among arachnids. The appearance of the phalanx is frightening and clearly does not encourage close acquaintance. Her body, 5–7 centimeters long, usually has a brownish-yellow color and is completely covered with
Zhdanovskaya phalanx
From the book Air Battle for the City on the Neva [Defenders of Leningrad against aces of the Luftwaffe, 1941–1944] author Degtev Dmitry MikhailovichZhdanovskaya phalanx In Leningrad, meanwhile, were preparing for defense. The situation that prevailed in the city now made everyone understand that the enemy was already at the gates. It was not regular units that were already sent to the front, but improvised units assembled from the world one by one. July 10
"Phalanx of Heroes"
From the book Literaturnaya Gazeta 6305 (No. 4 2011) author Literary Newspaper"Phalanx of Heroes" Legacy of the "Phalanx of Heroes" On the Moral and Aesthetic Experience of Decembrism Nikolay SKATOV, Corresponding Member of the Russian Academy of Sciences Decembrism is not only a social and political movement, not only a phenomenon national culture. Even apart from
Christ's phalanx
From the book Volume V. Book 1. Moral and ascetic creations the author Studit TheodoreChrist's phalanx My brethren, fathers and children. Do not be offended by the words with which I, humble, address you, for I do this constantly out of love for you and out of the most diligent care for you. Since I am your unworthy shepherd, I must fulfill my ministry and, as
"Phalanx"
From the book Domestic anti-tank systems author Angelsky Rostislav Dmitrievich"Phalanx" The Decree of 1957, along with work on the future "Bumblebee" complex, prescribed the implementation of topic No. 8, which also provided for the development of an infantry reactive anti-tank projectile with a light launcher with similar moderate characteristics for
lower limb
Bones lower limb are divided into four main groups: (1) foot, (2) lower leg, (3) thigh (femur), (4) hip joint. This chapter provides a detailed overview of radiographic anatomy and stacking for three of them: foot, lower leg, middle and distal femur, including ankle and knee joints.
FOOT
The bones of the foot are basically similar to the bones of the hand and wrist studied in Chapter 4. The 26 bones of one foot are divided into four groups.
Phalanges (toes) 14
Metatarsals (lift of the foot) 5
Tarsal bones 7
Phalanges of the toes
The distal part of the foot is represented by phalanges, forming fingers. The five toes of each foot are numbered 1 through 5 respectively, counting from the medial edge or from the big toe. Note that the first, or thumb, toe has only two phalanges, proximal and distal as well as the thumb. From the second to the fifth toes of each foot, in addition, they also have medial phalanx. Thus, two phalanges of the thumb and three in each finger from the second to the fifth make up 14 phalanx bones.
The similarity with the hand in this case is obvious, since each hand also has 14 phalanges. However, the phalanges of the foot are shorter than the phalanges of the hand, and their range of motion is significantly less.
When describing any bone or joint, it is necessary to indicate which finger and which foot they belong to. For example, the description - the distal phalanx of the first toe of the right foot - gives the exact localization of the bone.
The distal phalanges of the 2nd to 5th fingers are so small that it is rather difficult to see them on a radiograph as separate bones.
Metatarsal bones
Five metatarsus bones form the instep of the foot. They are numbered in the same way as the fingers, from one to five, counting from the medial edge to the lateral.
Three parts are distinguished in each metatarsal bone. The small rounded distal region is called head. The elongated thin middle part is called body. The slightly widened proximal end of each metatarsal is called basis.
Lateral department base of the fifth metatarsal has a prominent uneven tuberosity, which is the site of attachment of the tendon. The proximal fifth metatarsal and its tuberosity are usually clearly visible on radiographs, which is very important, since this area of the foot is often injured.
(5-6-7) 1, 2, 3 Cuneiformia
The resemblance of the tarsus to the analogous part of the upper limb is not so obvious, because the tarsus is represented by seven bones, as opposed to the eight bones of the wrist. At the same time, the bones of the tarsus are larger than the bones of the wrist, and less mobile, since they form the basis for maintaining the body in vertical position.
The seven bones of the tarsus are sometimes referred to as the bones of the ankle joint, although only one bone, the talus, belongs directly to this joint. Each of the bones of the tarsus will be further considered separately, together with all the bones with which it has articulations.
Calcaneus (calcaneus)
The heel bone is the largest and strongest bone in the foot. Its posterior lower part is formed by a well-defined process - calcaneal tubercle. Its uneven, rough surface is the site of attachment of muscle tendons. The lower expanded section of the tubercle passes into two small rounded processes: the larger lateral and the smaller, less commonly mentioned, medial branch.
On the lateral surface calcaneus is located fibular block, which can have a different size and shape and is visualized laterally in the picture in the axial projection. On the medial surface, in its anterior section, there is a large protruding process - support of the talus.
Articulations. The heel bone articulates with two bones: anterior section with cuboid and in the upper - with talus. Connection with the talus forms an important subtalar joint. Three articular surfaces are involved in this joint, providing a redistribution of body weight to maintain it in an upright position: this is an extensive posterior articular surface and two smaller ones anterior and medial articular surfaces.
Note that the median articular surface is top the protruding support of the talus, which provides medial support for this important support joint.
The depression between the posterior and middle articular surfaces is called calcaneal groove(Fig. 6-6). Combined With with a similar groove of the talus, it forms an opening for the passage of the corresponding ligaments. This hole, located in the middle of the subtalar joint, is called tarsal sinus(rice. 6-7).
Talus (talus)
The talus is the second largest bone in the tarsus and is located between the lower leg and the calcaneus. Together with the ankle and talocalcaneal joints, it is involved in the redistribution of body weight.
Articulations. The talus articulates with four bones: top with big and small tibia, from below with heel and front with scaphoid.
 |
Arches of the foot
Longitudinal arch of the foot. The bones of the foot form a longitudinal and transverse arch, providing a powerful spring-type support for the weight of the entire body. The springy longitudinal arch is formed by the medial and lateral components and is located for the most part at the medial edge and center of the foot.

The transverse arch runs along the plantar surface of the distal tarsus and tarsal-metatarsal joints. The transverse arch is formed mainly by the sphenoid bones, especially the short second, in combination with the largest sphenoid and cuboid bones (Fig. 6-9).
ANKLE JOINT
Front view
Ankle joint formed by three bones: two long bones of the lower leg, tibial and peroneal and one tarsal bone - the talus. The extended distal part of the thin fibula, which extends onto the talus, is called the external (lateral) ankle.
The distal part of the larger and more powerful tibia has an expanded articular surface for articulation with the same wide upper articular surface of the talus. The medial elongated process of the tibia, extended along the medial edge of the talus, is called the internal (medial) ankle.
Inner parts large and small tibia form a deep U-shaped depression, or joint space, covering the block of the talus from three sides. However, it is impossible to consider all three parts of the fissure in direct (posterior) projection, since the distal parts of the tibia and fibula are covered by the talus. This is because the distal fibula is somewhat posterior, as shown in the figures. Posterior projection with 15° inward rotation of the foot, called joint space projection 1 and shown in Fig. 6-15 allows full view of the open articular space above the talus.
anterior tubercle- a small expanded process, located laterally and anteriorly in the lower part of the tibia, articulates with the upper lateral part of the talus, while partially overlapping the fibula in front (Fig. 6-10 and 6-11).
Distal articular surface of the tibia forms the roof of the fork and is called tibial ceiling. In some types of fractures, especially in children and adolescents, there are injuries to the distal epiphysis and tibial ceiling.
Side view
On fig. 6-11 is a true lateral view of the ankle joint showing the distal fibula approximately 1 cm posterior to the tibia. This relative position becomes important in determining the true lateral laying of the lower leg, ankle joint and foot. The main mistake in lateral ankle placement is a slight rotation of the joint, as a result of which the medial and lateral ankles practically overlap each other. However, this will result in the ankle joint being depicted in an oblique view, as shown in the figures. Thus, with a true lateral projection lateral malleolus is located approximately 1 cm posterior from the medial malleolus. In addition, the lateral malleolus is also longer adjacent - medial approximately on the 1 cm (this is best seen in the frontal view, Fig. 6-10).
Axial (axial) view
An axial view of the inner edge of the distal fibula and tibia is shown in Fig. 6-12. The arch of the lower surface of the tibia (ceiling of the tibia) is shown in this figure from the inside, in the end projection of the ankle joint. You can also see the relationship lateral and medial malleolus fibula and tibia, respectively. smaller, fibula located more posteriorly. A line drawn through the center of both ankles is at an angle of approximately 15-20° to the frontal plane (parallel to the anterior surface of the body). Therefore, in order for the intermalleolar line to become parallel to the frontal plane, the lower leg and ankle
The leg joint should be rotated 15-20°. This relationship of the distal tibia and fibula is important when stacking the ankle joint or ankle slot in various projections, as described in the stacking sections of this chapter.
Ankle joint
The ankle joint belongs to the group synovial joints of the block type, in which only flexion and extensor movements are possible (dorsal flexion and plantar flexion). This is facilitated by strong collateral ligaments passing from the medial and lateral malleoli to the calcaneus and talus. Significant lateral pressure can cause an ankle sprain, accompanied by stretching or tearing of the lateral ligaments and rupture of the tendons of the muscles, which leads to an expansion of the intra-articular space on the side of the injury.
1 Frank ED et al: Radiography of the ankle mortise, Radiol Technol 62-65: 354-359, 1991.
 |
RADIOGRAPH EXERCISES
The radiographs of the foot and ankle presented in the three most common projections provide an anatomical overview of the bones and joints. To conduct a review test, it is proposed to name (or write out) all the parts marked on the pictures, closing the answers below.
Left foot, lateral view (Fig. 6-13)
A. Tibia.
B. Calcaneus.
B. Calcaneal tuberosity.
D. Cuboid bone.
D. Tuberosity of the fifth metatarsal bone.
E. Superimposed sphenoid bones. G. Navicular bone.
3. Subtalar joint. I. Talus.
Oblique projection of the right foot(rice. 6-14)
A. Interphalangeal joint of the first toe of the right foot.
B. Proximal phalanx of the first toe of the right foot.
B. Metatarsophalangeal joint of the first toe of the right foot.
G. Head of the first metatarsal bone.
D. Body of the first metatarsal bone. E. Base of the first metatarsal.
G. The second, or intermediate, sphenoid bone (partially overlapped by the first, or medial, sphenoid bone). 3. Navicular bone. I. Talus. K. Calcaneal tubercle. L. The third, or lateral, sphenoid bone. M. Cuboid bone.
H. Tuberosity of the base of the fifth metatarsal. A. The fifth metatarsophalangeal joint of the right foot. P. Proximal phalanx of the fifth toe of the right foot.
Projection of the joint space of the right ankle joint(Figure 6-15)
A. The fibula.
B. Lateral malleolus.
B. Open joint space of the ankle joint.
G. Talus.
D. Medial malleolus.
E. Lower articular surface of the tibia (articular surface of the epiphysis).
Lateral projection of the ankle joint(rice. 6-16)
A. The fibula.
B. Calcaneus.
B. Cuboid bone.
D. Tuberosity of the base of the fifth metatarsal. D. Navicular bone.
E. Talus. G. Tarsal sinus.
3. Anterior tubercle. I. Tibia.
SHIN - TIBIAN AND FIBULAR BONES
The following group of bones of the lower limb, which will be discussed in this chapter, includes two bones of the lower leg: tibia and fibula.
Tibia
The tibia is one of the largest bones of the human skeleton and serves as the supporting bone of the lower leg. It can be easily felt through the skin in the anteromedial part of the lower leg. It has three parts: central body and two ends.
proximal section. The expanded lateral sections of the upper, or proximal, end of the tibia form two powerful processes - medial and lateral condyle.
On the upper surface of the tibial head, between the two condyles, is located intercondylar eminence, in which two small tubercles are distinguished, medial and lateral intercondylar tubercles.
The superior articular surface of the condyles has two concave joint surfaces, often called tibial plateau, which form an articulation with the femur. On the lateral projection of the lower leg, it can be seen that the tibial plateau has a slope of 10° to 20° in relation to a line perpendicular to the long axis of the bone (Fig. 6-18) 1 . This important anatomical feature must be taken into account when laying to obtain a direct posterior projection of the knee joint, the central beam should be parallel to the plateau and perpendicular to the cassette. In this case, the joint space will appear open in the picture.
In the proximal part of the bone on its anterior surface, immediately behind the condyles, there is a rough protrusion - tuberosity of the tibia. This tuberosity is the site of attachment of the patellar ligament, which includes the tendons of the large muscle of the anterior surface of the thigh. Occasionally, adolescents experience separation of the tibial tuberosity from the body of the bone, a condition known as Osgood-Schlatter disease(see clinical indications, p. 211).
The body of the tibia is the long middle part of the bone, located between its two ends. On the anterior surface of the body, between the tibial tuberosity and the medial malleolus, there is a pointed crest, or cutting edge tibia, which is well palpable under the skin.
Diet department. The distal tibia is smaller than the proximal, it ends with a short pyramidal process, medial malleolus, which can be easily palpated in the medial region of the ankle joint.
On the lateral surface of the lower end of the tibia is a flat, triangular fibular notch, to which the lower end of the fibula adjoins.
Fibula
The fibula is smaller and laterally posterior relative to the larger tibia. The upper, or proximal, section of the bone forms an expanded head, which articulates with the outer surface of the posterior inferior part of the lateral condyle of the tibia. The upper end of the head is pointed, it is called tip head of the fibula.
Body The fibula is the long thin part between its two ends. Expanded distal fibula
1 Manaster Bj: handbooks in radiology, ed. 2, Chicago, 1997, Year Book Medical Publishers, Inc.
 |
FEMUR
The thigh, or femur, is the longest and most powerful of all the tubular bones of the human skeleton. It is the only long bone between the hip and knee joints. The proximal femur will be described in chapter 7 along with the hip joint and pelvic bones.
Middle and distal femur, anterior view(rice. 6-19)
Like all tubular bones, the body of the femur is an elongated and thinner part. On the front surface of the lower part of the femur lies the patella, or patella. The patella, the largest sesamoid bone of the skeleton, is located anterior to the distal femur. Note that in the frontal view, with the leg fully extended, the lower edge of the patella is approximately 1.25 cm above, or proximal to, the actual knee joint. It is important to keep this in mind when laying the knee joint.
A small, smooth, triangular depression on the anterior surface of the lower femur is called the patella (Fig. 6-19). This depression is also sometimes called the intercondylar sulcus. The literature also contains the definition of a block furrow (meaning a block-shaped formation resembling a spool of thread, which is made up of the medial and lateral condyles with a depression between them). It is necessary to know all three terms as referring to this recess.
With a straightened leg, the patella is located slightly above the patella surface. Lying in the thickness of the tendon of the muscle, the patella with a bent knee moves down, or distally, along the patella surface. This is clearly seen in Fig. 6-21, p. 204, which shows the knee joint in lateral view.
Middle and distal femur, posterior view (Fig. 6-20)
On the posterior surface of the distal femur, two rounded condyles are visible, separated in the distal posterior region by a deep intercondylar fossa, or notch, over which the popliteal surface is located (see p. 204).
In the distal parts of the medial and lateral condyles, there are smooth articular surfaces for articulation with the tibia. With the femur in a vertical position, the medial condyle is located slightly below, or distal to, the lateral (Fig. 6-20). This explains why the CL should be tilted 5-7° cranially when performing a lateral projection of the knee joint, which projects the condyles on top of each other, and the femur is parallel to the cassette. An explanation for this is given additionally in Fig. 6-19, which shows that in a vertical anatomical position, when the condyles of the distal femur are parallel to the lower plane of the knee charter, the body of the femur in an adult is deviated from the vertical by about 10 °. The value of this angle ranges from 5° to 15°". In people of small stature with a wide pelvis, this angle will be greater, and in tall patients with narrow pelvis, respectively, less. Thus, the value of this angle in women, as a rule, is greater than in men.
A characteristic difference between the medial and lateral condyles is the presence of the adductor tubercle, a slightly protruding area to which the adductor tendon attaches. This tubercle is located in the back
Keats TE et al: radiology, 87:904, 1966.
Patella
Patella(patella) - a flat triangular bone, about 5 cm in diameter. The patella appears upside down because its pointed tip forms the inferior edge, but rounded base- upper. Outer side front surface convex and rough, and the inner oval back surface, articulating with the femur - smooth. The patella protects the front of the knee joint from injury, in addition, it plays the role of a lever that increases the lifting force of the quadriceps femoris, the tendon of which is attached to the tuberosity of the tibia of the tibia. The patella in its upper position with a fully extended limb and a relaxed quadriceps muscle is a mobile and easily displaced formation. If the leg is bent at the knee joint, and the quadriceps muscle is tense, the patella moves down and is fixed in this position. Thus, it can be seen that any displacement of the patella is associated only with the femur, and not with the tibia.
KNEE-JOINT
The knee joint is a complex articulation that includes, first of all, tibiofemoral the joint between the two condyles of the femur and their corresponding condyles of the tibia. Also involved in the formation of the knee joint femoral-patellar- nickname joint, since the patella articulates with the anterior surface of the distal femur.
Menisci (articular discs)
The medial and lateral menisci are flat intra-articular cartilaginous discs between the upper articular surface of the tibia and the condyles of the femur (Fig. 6-27). The menisci are crescent-shaped, their thickened peripheral edge gently descends towards the thinned central part. The menisci are a kind of shock absorbers that protect the knee joint from shock and pressure. It is believed that the menisci, together with the synovial membrane, are involved in the production of synovial fluid, which plays the role of lubricating the articular surfaces of the femur and tibia, covered with elastic and smooth hyaline cartilage.
I L A V A O
LOWER LIMB
AP posterior tibia (Fig. 6-29)
A. Medial condyle of the tibia.
B. Body of the tibia.
B. Medial malleolus.
G. Lateral malleolus.
D. The body of the fibula. E. The neck of the fibula. G. The head of the fibula. 3. Apex (styloid process) of the head of the fibula
I. Lateral condyle of the tibia. K. Intercondylar eminence (tibial crest
Lateral Leg View (Fig. 6-30)
A. Intercondylar eminence (tibial crest)
bones).
B. Tuberosity of the tibia.
B. Body of the tibia.
D. The body of the fibula.
D. Medial malleolus. E. Lateral malleolus.
Front posterior view of the knee joint (Fig. 6-31)
A. Medial and lateral intercondylar tubercles; you
stupas of the intercondylar eminence (greater ridge
calf bone).
B. Lateral epicondyle of the thigh.
B. Lateral condyle of the thigh.
G. Lateral condyle of the tibia. D. Upper articular surface of the tibia.
E. Medial condyle of the tibia. G. Medial condyle of the thigh.
3. Medial epicondyle of the thigh.
I. Patella (visible through the femur).
Lateral view of the knee joint (Fig. 6-32)
A. Base of the patella.
B. Apex of the patella.
B. Tibial tuberosity.
G. The neck of the fibula.
D. The head of the fibula. E. Apex of the head (styloid process) of the fibula
bones. G. Medial and lateral condyles superimposed on each other
3. Patellar surface (intercondylar, or block, furrow).
Lateral view of the knee joint (with slight rotation) (Fig. 6-33)
I. Hillock of the adductor muscle. K. Lateral condyle. L. Medial condyle.
Tangential View (femoral-patellar joint) (Fig. 6-34)
A. Patella.
B. Femoral-patellar joint.
B. Lateral condyle.
D. Patellar surface (intercondylar, or block, furrow). D. Medial condyle.
The only exception to the group of synovial joints is distal tibiofibular joint, related to fibrous compounds, in which the articulation between the articular surfaces of the tibia and fibula occurs with the help of connective tissue. It refers to syndesmoses and is continuous motionless, or sedentary, articulation (amphiarthrosis). The most "distal" part of this joint is smoothed and covered by a common synovial membrane of the ankle joint.
 |
SURFACES AND PROJECTIONS OF THE FOOT Surfaces. Determining the surface of the foot can sometimes cause some difficulty, since the foot has rear called top part. The dorsum usually refers to the back of the body. In this case, it means back of the foot, which is the upper, or opposite sole, surface. The sole of the foot is back, or plantar, surface.
Projections. Posterior projection of the foot is an plantar projection. Less commonly used anterior projection may also be called rear projection. Radiologists should be familiar with each of these terms and be well aware of which projection they are performing.
STYLING
General issues
Radiography of the lower extremity is usually performed on an imaging table, as shown in Fig. 6-38. Patients with severe trauma are often examined directly on a stretcher or gurney.
DISTANCE
The x-ray source/receiver distance (RSD) for x-rays of the lower extremity is usually 100 cm. lift extra. For X-rays on a gurney or stretcher, use the gauge, usually located on the deep diaphragm of the machine, to set RIP = 100 cm.
Radiation protection
When radiography of the lower extremity gonadal protection is desirable, as the gonads are in close proximity to the radiation area. The gonadal area can be protected with any leaded vinyl cape 1 . And although the requirements for radiation protection of the gonads are applicable only to patients of reproductive age and only when the gonads are directly located in the area of the direct beam, it is recommended to apply it in all cases.
IRISING
The iris rules are always the same - the boundaries of the iris area should be visible from all four sides of the image, but the images of the organs under study should not be cut off. A cassette should be used that is as small as possible to image the region of interest. It should be noted that small-sized cassettes are most often used for radiography of the lower extremity.
Several projections can be made on one cassette during radiography of the lower limb, so you should be careful about diaphragming.
When using digital x-ray imagers (particularly computerized x-ray systems with storage phosphor plates), cover the unused area of the cassette with a sheet of leaded vinyl. The phosphor is very sensitive to stray radiation, which can cause severe fogging on subsequent radiographs.
If the aperture limits are visible from all four sides, then this makes it easier to find the center of the image - at the intersection of the diagonals.
GENERAL INSTALLATION PRINCIPLES
For the upper and lower limbs, the same rule applies when laying - the long axis of the examined limb should

Rice. 6-38. Exemplary laying for the mediolateral projection of the lower limb:
Correct direction of the central line;
Correct aperture;
Correct use radiation protection;
Diagonal laying of the lower limb allows you to get on
X-ray image of both joints
to be located along the long axis of the cassette. If you need to perform several projections, then when taking multiple images on one cassette, the orientation of the limb must be preserved.
An exception is the shin of an adult. It is usually laid diagonally across the cassette so that the knee and ankle joints enter, as shown in Fig. 6-38.
CORRECT CENTERING
Accurate centering and positioning of the body part to be examined, as well as the correct direction of the CL, are very important when X-raying the upper and lower extremities. The images should show open joint spaces and there should be no geometric distortion of the shape of the bones, that is, the part of the body being removed should be parallel to the plane of the cassette, and the CL should be directed perpendicular to the removed limb. Follow the directions on the installation pages.
EXPOSURE PARAMETERS
Exposure parameters for radiography of the lower extremity:
1. Low or medium kV (50-70).
2. Short exposure time.
3. Small focus.
Correctly exposed radiographs of the lower extremity should show both soft tissue contours and clear trabecular bone structure.
RADIOGRAPHY IN PEDIATRICS
First, the child should be spoken to in a language he understands. Parents often help with restraining the child, especially if it is not a case of trauma. At the same time, care must be taken to radiation protection. Retainers are useful in many cases, as they help the child to keep the limb still in the desired position. Soft cushions for ease of styling and straps for fixation are common tools. Sand pads should be used carefully as they are heavy. Body thickness measurement is an important factor in determining optimal exposure parameters.
In general, reduced exposure parameters are used in pediatrics due to the small size and low density of the extremities being examined. use short times exposure by increasing the current (mA) - this reduces the dynamic blur of the image.
RADIOGRAPHY IN GERIATRICS
Elderly patients should be positioned for imaging with caution, and radiography of the lower extremity is no exception. Look out for signs of a hip fracture (leg overturned). Routine styling should be adjusted for the patient's ability to bend the limbs and for personal pathology. Cushions and braces should be used when positioning the limb to ensure patient comfort.
Exposure parameters should be selected taking into account possible osteoporosis or osteoarthritis. Short exposure times are used, increasing the current (mA), this reduces the dynamic blur of the image due to arbitrary and involuntary movements.
ARTHROGRAPHY
Arthrography is commonly used to visualize large synovial joints such as the knee. It is performed by inserting into the joint cavity contrast agents under sterile conditions. Arthrography reveals diseases and injuries of the menisci, ligaments and tendons (see Chapter 21).
RADIONUCLIDE DIAGNOSIS
Radionuclide scanning is intended for the diagnosis of osteomyelitis, bone metastases, impacted fractures, as well as inflammatory diseases subcutaneous tissue. The evaluation of the studied organ is carried out within 24 hours from the start of the study. A radionuclide study is more informative than radiography, since it allows you to evaluate not only the anatomical, but also the functional state of the organ.
Clinical indications
Radiologists should be familiar with the most common clinical indications for lower extremity radiography, which are (the list below is not exhaustive):
Bone cysts- benign tumor-like formations, which are a cavity filled with serous fluid. They often develop in children and are located mainly in the area of the knee joint.
Chondromalacia patella- often called runner's knee. Pathology is based dystrophic changes(softening) of cartilage, leading to wear; accompanied by pain and constant irritation of the affected area. Runners and cyclists are often affected.
Chondrosarcoma- malignant tumor bones. The predominant localization is the pelvis and long tubular bones. It is more common in men over 45 years of age.
Ewing's sarcoma- primary malignant tumor of the bone, as a rule, is observed in childhood, from 5 to 15 years. The tumor is usually localized in the diaphysis of long tubular bones. V clinical picture pain, fever at the onset of the disease and leukocytosis are noted.
Exostosis, or osteochondroma- a benign tumor-like lesion of the bone, the essence of which lies in the hyperproduction of the bone substance (often the area of the knee joint is affected). The tumor grows in parallel with the growth of the bone, while moving away from the adjacent joint.
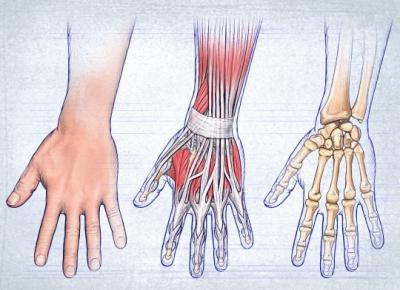
On closer examination, the structure, like any other department of our musculoskeletal system, is quite complex. It is made up of three main structures: bones, muscles, and ligaments that hold the bones together. There are three sections in the hand, namely, the wrist, fingers, and metacarpus.
In this article, we will take a closer look at the hand: the joints of the hand. Let's start with a description of the bones in its various departments.
wrist bones
Since the hands must perform fairly precise and intricate movements, the structure of the bones of the hand is also extremely complex. In the wrist - 8 small bones of irregular shape, arranged in two rows. In the figure below you can see the structure of the right hand.
The proximal row forms an articular surface convex to the radius. It includes bones, if you count from the fifth to the thumb: pisiform, trihedral, lunate and scaphoid. The next row is the distal one. It connects to an irregularly shaped proximal joint. The distal row consists of four bones: trapezius, polygonal, capitate and hamate.
Metacarpal bones
This department, consisting of 5 tubular ones, also demonstrates the intricate structure of the hand. The skeleton of these tubular bones is complex. Each of them has a body, base and head. The 1st finger is shorter than the others and is massive. The second metacarpal is the longest. The rest decrease in length as they move away from the first and approach the ulnar edge. The bases of the aforementioned metacarpus bones articulate with the bones that form the wrist. The first and fifth metacarpals have bases with saddle-shaped articular surfaces, the others are flat. The heads of the metacarpal bones, which have an articular surface (hemispherical), articulate with the proximal digital phalanges.
Finger bones

Each finger, with the exception of the first, which consists of only two phalanges and does not have a middle one, has 3 phalanges: distal, proximal and middle (intermediate). The shortest - distal; proximal - the longest. At the distal end, there is a head of the phalanx, and at the proximal end, its base.
Sesamoid bones of the hand
In the thickness of the tendons, in addition to these bones, there are sesamoid, located between the proximal phalanx of the thumb and its metacarpal bone. There are also unstable sesamoid bones. They are located between the proximal phalanges of the fifth and second fingers and their metacarpals. Usually sesamoid bones are located on the palmar surface. But sometimes they can be found on the back. The pisiform bone also belongs to the above species. The sesamoid bones and their processes increase the leverage of the muscles attached to them.
We examined the structure of the hand and the bones of the hand, now we turn to the ligamentous apparatus.
wrist joint
It is made up of the radius and the bones of the proximal row of the wrist: trihedral, lunate and navicular. The ulna is complemented by the articular disc and does not reach the wrist joint. The main role in the formation of the elbow joint plays Whereas the wrist - radial. The wrist joint is elliptical in shape. It allows abduction, adduction of the hand, flexion and extension. A small passive rotational movement (by 10-12 degrees) is also possible in this joint, but is carried out due to the elasticity of the articular cartilage. Across soft tissues it is easy to detect the gap of the wrist joint, which is palpable from the ulnar and radial sides. With the ulna, you can feel the depression between the triquetral bone and the head of the ulna. On the radial side - a gap between the navicular bone and the lateral styloid process.
The movements of the wrist joint are closely related to the work of the mid-carpal joint, located between the distal and proximal rows. Its surface is complex, irregular in shape. With flexion and extension, the range of mobility reaches 85 degrees. Adduction of the hand in the above-mentioned joint reaches 40 degrees, abduction - 20. The wrist joint can perform circumduction, i.e. Roundabout Circulation.
This joint is reinforced by numerous ligaments. They are located between individual bones, as well as on the lateral, medial, dorsal and palmar surfaces of the wrist. (radial and ulnar) play the most important role. On the ulnar and radial sides, between the bone elevations, there is a flexor retinaculum - a special ligament. In fact, it does not apply to the joints of the hand, being a thickening of the fascia. The flexor retinaculum converts the carpal groove into a canal through which the median nerve and flexor tendons of the fingers pass. Let's continue to describe anatomical structure hands.
Carpometacarpal joints
They are flat and immobile. The exception is the joint of the thumb. The range of motion of the carpal-metacarpal joints is no more than 5-10 degrees. They have limited mobility, because the ligaments are well developed. Located on the palmar surface, they form a stable palmar ligamentous apparatus that connects the bones of the wrist and metacarpals. There are arcuate ligaments on the hand, as well as transverse and radial ligaments. The capitate bone is central in the ligamentous apparatus, ligaments are attached to it. Palmar developed much better than the back. The dorsal ligaments connect the bones of the wrist. They form thickenings of capsules that cover the joints between these bones. Interosseous are located in the second row of carpal bones.
In the thumb, the carpometacarpal joint is formed by the base of the first metacarpal and polygonal bone. The articular surfaces are saddle-shaped. This joint can perform the following actions: abduction, adduction, reposition (reverse movement), opposition (opposition) and circumduction (circular movement). The volume of grasping movements, due to the fact that the thumb is opposed to all the others, increases significantly. 45-60 degrees is the mobility of the carpometacarpal joint of this finger during adduction and abduction, and during reverse movement and opposition - 35-40.

The structure of the hand: metacarpophalangeal joints
The named joints of the hand are formed by the heads of the metacarpal bones with the participation of the bases of the proximal phalanges of the fingers. They are spherical in shape, have 3 axes of rotation perpendicular to each other, around which extension and flexion, abduction and adduction are carried out, as well as circular motions(circumduction). Adduction and abduction is possible at 45-50 degrees, and flexion and extension - at 90-100. These joints have collateral ligaments located on the sides that strengthen them. The palmar, or accessory, are located on the palmar side of the capsule. Their fibers are intertwined with the fibers of the deep transverse ligament, which prevents the heads of the metacarpal bones from diverging in different directions.
Interphalangeal joints of the hand
They are block-shaped, and their axes of rotation run transversely. Extension and flexion is possible around these axes. Proximal interphalangeal joints have a flexion and extension volume of 110-120 degrees, distal - 80-90. The interphalangeal joints are very well reinforced thanks to the collateral ligaments.
Synovial, as well as fibrous sheaths of the tendons of the fingers
The extensor retinaculum, like the flexor retinaculum, plays a huge role in strengthening the position of the tendons of the muscles passing under them. This is especially true when the hand is working: when it is extended and flexed. Nature has conceived a very competent structure that finds support in the above-mentioned ligaments from their inner surface. The separation of the tendons from the bones prevents ligaments. This allows for intense work and strong muscle contraction to withstand great pressure.
Special tendon sheaths, which are bone-fibrous or fibrous channels, contribute to reducing friction and sliding of the tendons going to the hand from the forearm. They have synovial sheaths. Their largest number (6-7) is located under the extensor retinaculum. The radius and ulna have grooves that correspond to the location of the tendons of the muscles. As well as the so-called fibrous bridges, which separate the channels from each other and pass to the bones from the extensor retinaculum.

Palmar synovial sheaths belong to the flexor tendons of the fingers and hands. The common synovial sheath extends to the center of the palm and reaches the distal phalanx of the fifth finger. Here are the tendons of the superficial and deep flexors of the fingers. The thumb has a long flexor tendon located separately in the synovial sheath and passing to the finger along with the tendon. The synovial sheaths in the palm area are devoid of the tendon of the muscles that go to the fourth, second and third fingers. Only the tendon of the fifth finger has a synovial sheath, which is a continuation of the general one.
Muscles of the hand
In the figure below you can see the muscles of the arm. The structure of the hand is shown here in more detail.

The muscles in the hand are only on the palmar side. They are divided into three groups: middle, thumb and small fingers.
Since the movements of the fingers require great precision, there are a significant number of short muscles in the hand, complicating the structure of the hand. The muscles of the hand of each of the groups will be considered below.
Middle muscle group
It is formed by worm-like muscles, starting from the tendons of the deep flexor of the fingers and attached to the proximal phalanges, or rather their bases, from the second to the fifth finger, if we consider the structure of the hand. These muscles of the hand also come from the dorsal and palmar interosseous, located in the spaces between the bones of the metacarpus, attached to the base of the proximal phalanges. The function of this group is that these muscles are involved in the flexion of the proximal phalanges of these fingers. Thanks to the palmar interosseous muscles, it is possible to bring the fingers to the middle finger of the hand. With the help of the dorsal interosseous, they are diluted to the sides.
Muscles of the thumb

This group forms the eminence of the thumb. These muscles begin near the nearby bones of the metacarpus and wrist. As for the thumb, its short flexor is attached near the sesamoid bone, which is located near the base of the proximal phalanx. The opposing thumb muscle goes to the first metacarpal bone, and the adductor thumb muscle is located on the side of the internal sesamoid bone.
Muscles of the thumb
This group of muscles forms an elevation on the inside of the palm. These include: the abductor of the little finger, the opposing little finger, the short palmar, and the short flexor.
They originate from nearby bones in the wrist. These muscles are attached to the base of the fifth finger, more precisely its proximal phalanx, and to the fifth metacarpal bone. Their function is reflected in the name.
In the article, we tried to most accurately represent the structure of the hand. Anatomy is a fundamental science, requiring, of course, a more thorough study. Therefore, some questions remained unanswered. The structure of the hand and wrist is a topic that is of interest not only to physicians. Knowledge of it is also necessary for athletes, fitness instructors, students and other categories of people. The structure of the hand, as you noticed, is quite complex, and you can study it for quite some time, relying on various sources.